This study included eight participants ranging from 22–29 years of age. Table 1 describes how to calculate the distance to obtain each degree of eccentricity from the center of the macula. Table 2 provides the demographics of the participants. The study sample includes an equal number of males and females with a wide variety of ethno-racial diversity. Table 3 shows the mean results of MPOD obtained by both the devices and L-OD and Z-OD of all participants involved in the study at various eccentricities. The mean MPOD and standard deviation obtained by the heterochromatic flicker photometer and the reflectometry technique was 0.480 (SD 0.14) and 0.593 (SD 0.161) respectively. There was excellent correlation between the MPOD measurement obtained using the techniques with Person correlation coefficient r = 0.92 (p < 0.001). The Z-OD was larger centrally compared to the L-OD measured in the foveal region. The L-OD to Z-OD ratio centrally was 1:2.61. The Z-OD decreased as a function of eccentricity at the center of the fovea. At 1 degree from the central fovea the concentration of Z-OD measured by reflectometry decreased significantly, with an increase in L-OD. The L-OD to Z-OD ratio at 1 degree from central fixation was 1.38:1.0. In the parafoveal region at 2 degrees from central fixation the lutein became the predominant carotenoid and the L-OD to Z-OD ratio was 2.08:1.0. Tables 4, 5, and 6 show the data obtained from all eight subjects. Examining the tables, it is obvious that there is significant interindividual variability of L-OD, Z-OD, and MPOD values, indicating that the physiological limits of normality can be large.
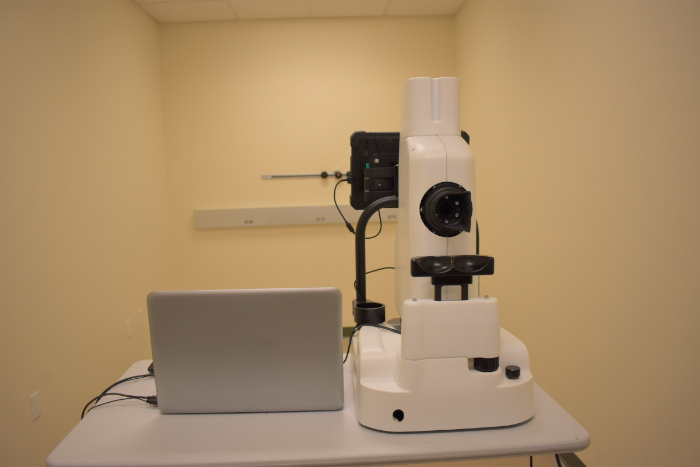
Figure 1: Macular pigment reflectometer. Macular Pigment Reflectometer used in this experiment. Please click here to view a larger version of this figure.
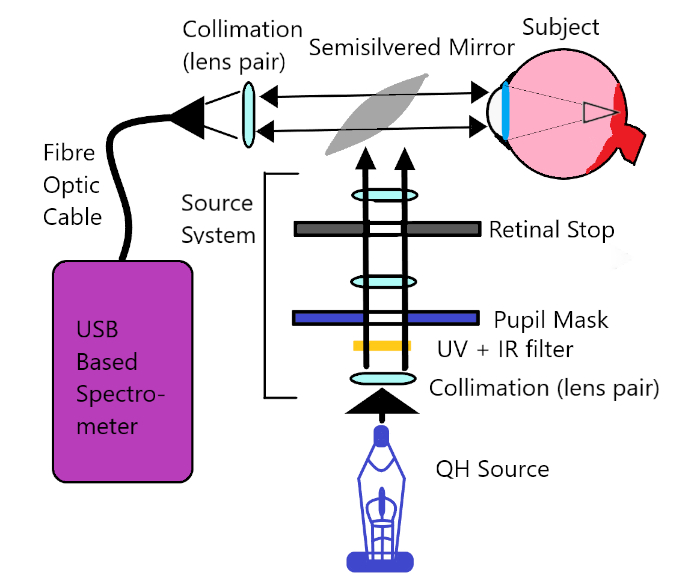
Figure 2: Macular pigment reflectometer operational schematic. Diagram of the internal operational schematics of the MPR device. Please click here to view a larger version of this figure.
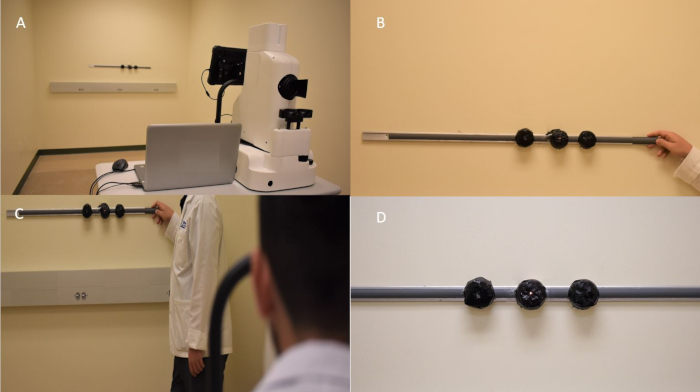
Figure 3: Peripheral measurement track system. (A) The macular pigment reflectometer with the peripheral track system 6.1 m away. (B) The track system with a researcher pointing at the 0 degree LED light. (C) The whole system as it would appear when the participant is being tested. (D) The track system with the 1 degree LED light on. Please click here to view a larger version of this figure.
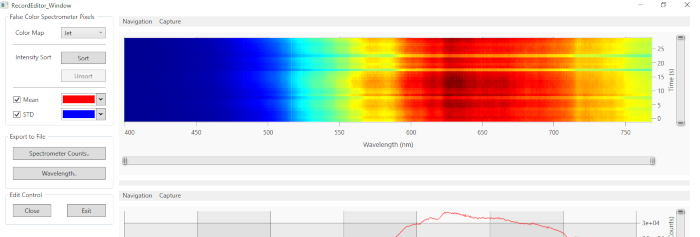
Figure 4: Window showing slide bars used for editing measurements to desired time. The slide bars used to edit the desired time frame. The image shows the first 10 s being removed. Please click here to view a larger version of this figure.
| Test distance [m] | 3 | 4 | 5 | 6.1 | 7 | 8 | 9 | 10 |
| Distance between lights [m] | 0.052 | 0.07 | 0.087 | 0.107 | 0.122 | 0.14 | 0.157 | 0.175 |
Table 1: Separation between fixation lights at various distances from target. The distance between the lights is the value for x in this equation:

where d is the test distance.
| Subject | Age | Gender | Ethnicity | Race |
| 3002 | 27 | F | Hispanic | Caucasian/More than one race |
| 3003 | 28 | F | Hispanic | None |
| 3004 | 26 | F | Not Hispanic | African American |
| 3005 | 24 | M | Hispanic | Asian/More than one race |
| 3006 | 27 | M | Not Hispanic | Asian |
| 3007 | 25 | F | Not Hispanic | African American |
| 3009 | 29 | M | Hispanic | Caucasian/More than one race |
| 3010 | 22 | M | Not Hispanic | Asian |
Table 2: Demographics of participants of the study. Table shows the age, gender, and ethnicity of the tested participants. The average age of the participants was 26. There was a 1:1 ratio of men to women. The self-identified ethnicity of the participants included 50% Hispanic and about 37.5% of either Asian or More Than One Race.
| Mean L-OD | Mean Z-OD | Mean-reflectometry MPOD | Mean Z-L Ratio | Mean-Flicker photomettry MPOD | |
| Central | 0.247 | 0.425 | 0.593 | 2.61:1 | 0.48 |
| Peripheral 1 deg | 0.402 | 0.122 | 0.248 | 1:1.38 | Not available |
| Peripheral 2 deg | 0.366 | 0.03 | 0.143 | 1:2.08 | Not available |
Table 3: Mean values of carotenoids at various eccentricities. The table shows the mean results from the eight participants in the study. SD for mean central L-OD (0.188) and mean central Z-OD (0.142). SD for Mean Central MPOD of MPR (0.161) and SD for Mean Central MPOD of the reflectometer (0.14). SD for mean L-OD at peripheral 1 degree (0.224) and mean Z-OD at peripheral 1 degree (0.122). SD for mean MPOD of MPR at peripheral 1 degree (0.248). SD for mean L-OD at peripheral 2 degree (0.366) and SD for mean Z-OD at peripheral 2 degree (0.030). SD for mean MPOD of MPR at peripheral 2 degree (0.143).
| Participant | L-OD | Z-OD | MPOD | Z-L Ratio | MPS |
| 3002 | 0.525 | 0.409 | 0.669 | 0.778 | 0.58 |
| 3003 | 0.566 | 0.415 | 0.6525 | 0.733 | 0.48 |
| 3004 | 0.1615 | 0.291 | 0.437 | 1.793 | 0.437 |
| 3005 | 0.121 | 0.414 | 0.555 | 3.432 | 0.555 |
| 3006 | 0.148 | 0.724 | 0.888 | 4.892 | 0.888 |
| 3007 | 0.074 | 0.389 | 0.536 | 5.257 | 0.536 |
| 3009 | 0.197 | 0.26 | 0.361 | 1.32 | 0.361 |
| 3010 | 0.183 | 0.496 | 0.642 | 2.71 | 0.642 |
Table 4: Individual carotenoid optical density measurements obtained at central fixation. Table shows the measurements obtained at central fixation for all eight participants.
| Participant | L-OD | Z-OD | MPOD | Z-L Ratio |
| 3002 | 0.325 | 0 | 0.012 | 0 |
| 3003 | 0.385 | 0.08 | 0.166 | 0.208 |
| 3004 | 0.121 | 0.253 | 0.392 | 2.091 |
| 3005 | 0.7015 | 0 | 0.119 | 0 |
| 3006 | 0.362 | 0.286 | 0.45 | 0.79 |
| 3007 | 0.104 | 0.265 | 0.391 | 2.548 |
| 3009 | 0.589 | 0 | 0.183 | 0 |
| 3010 | 0.626 | 0.094 | 0.273 | 0.15 |
Table 5: Individual carotenoid optical density measurements obtained at 1 degree from central fixation. Table shows the measurements obtained at 1 degree from central fixation for all eight participants.
| Participant | L-OD | Z-OD | MPOD | Z-L Ratio |
| 3002 | 0.146 | 0 | 0.043 | 0 |
| 3003 | 0.351 | 0 | 0.066 | 0 |
| 3004 | 0.063 | 0.077 | 0.169 | 1.222 |
| 3005 | 0.189 | 0.017 | 0.067 | 0.09 |
| 3006 | 0.902 | 0 | 0.291 | 0 |
| 3007 | 0.04 | 0.099 | 0.201 | 2.475 |
| 3009 | 0.718 | 0.046 | 0.232 | 0.064 |
| 3010 | 0.518 | 0 | 0.076 | 0 |
Table 6: Individual carotenoid optical density measurements obtained at 2 degrees from central fixation. Table shows the measurements obtained at 2 degrees from central fixation for all eight participants.
