Briefly summarized, human whole blood was collected in heparin-loaded monovettes then pooled and used to evaluate the baseline levels of cell counts as well as plasmatic hemocompatibility markers.
Subsequently, the tubing containing the neurovascular implant samples was filled, and the blood was perfused for 60 min at 150 mL/min and 37 °C using a peristaltic pump. Again, the number of cells was analyzed in all groups, and the plasma samples were prepared for ELISA analyses (Figure 1). The quantification of the blood cells and blood parameters, such as hemoglobin and hematocrit, was performed directly after blood collection as well as after perfusion in the flow loop model for all sample types and the control. No changes were detected regarding the number of WBCs (Figure 2A), RBCs (Figure 2B), or the hematocrit values (Figure 2C). However, a decrease in hemoglobin levels was detected after the incubation of blood in the flow loop model when compared to the baseline values, which was due to the perfusion of blood in the flow loop system (Figure 2D). In addition, a decrease in platelet numbers was observed due to blood perfusion. Furthermore, this effect was increased when an uncoated stent was present in the tubing, indicating the adhesion of platelets to the biomaterial. Nonetheless, it was clearly demonstrated that the loss of platelets was significantly higher when the uncoated stent was incubated with blood, as opposed to the fibrin-heparin-coated stent (Figure 2E).
Potential alterations of the hematologic plasma markers were also investigated in the test groups after perfusion and compared to the baseline values of the freshly drawn blood. The TAT complex concentration, which reflects the activation status of the coagulation system, was mildly increased due to blood perfusion (Figure 3A). In the bare metal stent group, however, a significant increase in the TAT was detected, indicating a profound activation of the coagulation system. The fibrin-heparin-coated stent prevented the activation of the coagulation system, since no increase in the TAT was determined.
The perfusion led to an increased activation of the complement cascade, which was determined by measuring SC5b-9 (Figure 3B). However, incubation with uncoated or fibrin-heparin-coated stents did not further increase the SC5b-9 concentration. Similar results were obtained when analyzing the activation of the neutrophil granulocytes through the quantification of PMN-elastase concentrations (Figure 3C).
Visualization of the stent surface was performed using SEM. Clear differences between the two stent groups were detected after blood incubation. While on the surface of the uncoated stent a dense network of blood cells and proteins was present, no adhesion of proteins or cells was detected on the surface of the fibrin-heparin-coated stent (Figure 4).
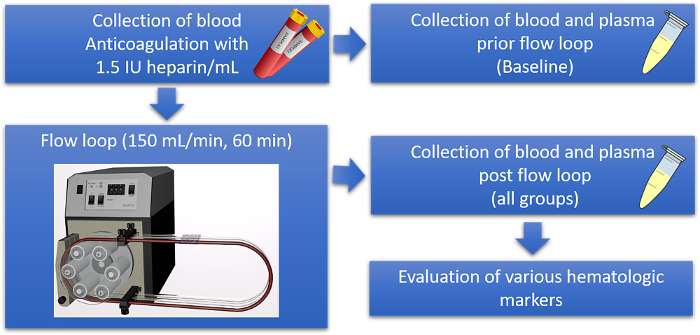
Figure 1: Schematic overview of the hemocompatibility evaluation of stents in a well-established flow loop model. Fresh human whole blood is collected from healthy donors in blood tubes containing heparin for anticoagulation. For each donor, an empty tube as well as tubes preloaded with the sample material are subsequently filled with fresh blood and incubated in the flow loop at a rate of 150 mL/min at 37 °C for 60 min. Additionally, plasma samples are prepared from freshly drawn blood to obtain the baseline values of each donor. After the incubation, the plasma samples from the test tubing, with and without sample materials, are prepared and analyzed using a specific ELISA. Please click here to view a larger version of this figure.
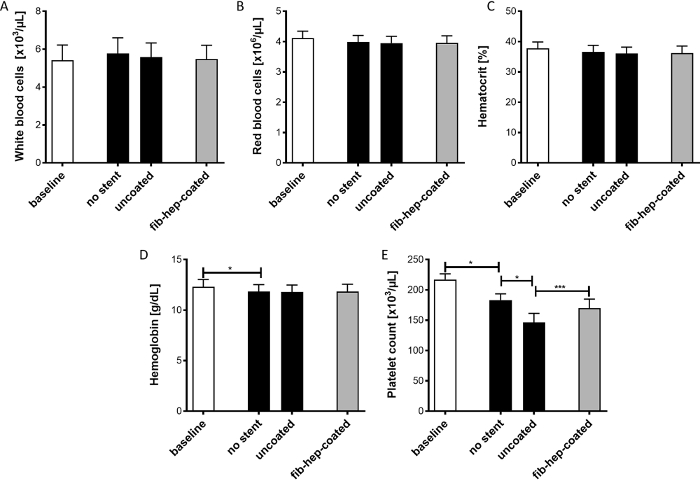
Figure 2: Analysis of different cell types and blood parameters before and after incubation of different stent implants in the flow loop model. The determination of white blood cells (A), red blood cells (B), hematocrit (C), hemoglobin (D), and platelets (E) was performed. The data are displayed as mean ± SEM (n = 5, p* < 0.5, p*** < 0.001). Please click here to view a larger version of this figure.
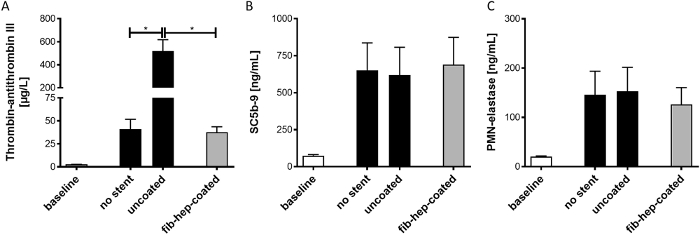
Figure 3: Determination of platelet or immune system activation markers before and after incubation with neurovascular implants. The markers for the (A) activation of blood coagulation (TAT), (B) complement system (SC5b-9), and (C) neutrophils (PMN-elastase) were quantified using ELISA. The analysis was performed on plasma samples gained from freshly drawn blood or blood incubated with different stents in the flow loop model. The data are displayed as mean ± SEM (n = 5, p* < 0.5). Please click here to view a larger version of this figure.
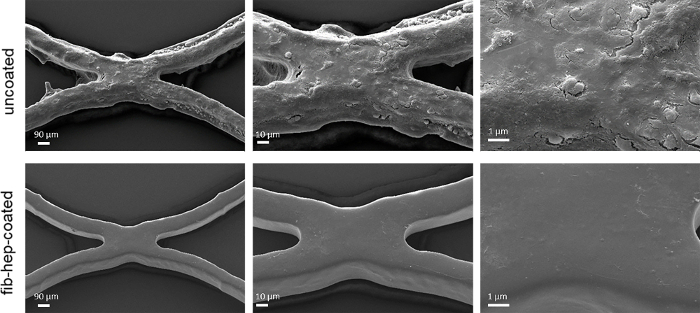
Figure 4: Scanning electron microscopic analysis of stents after incubation with blood. The aggregation of blood plasma proteins and platelets on uncoated stent material was observed. In comparison, stent materials with the fibrin-heparin coating did not demonstrate adhesion of cells or other blood components on the surface (magnification of 500-, 1,000-, and 2,500-fold). Please click here to view a larger version of this figure.
