A Reproducible Intensive Care Unit-Oriented Endotoxin Model in Rats
Summary
Here, we present a reproducible intensive care unit-oriented endotoxin model in rats.
Abstract
Sepsis and septic shock remain the leading cause of death in intensive care units. Despite significant improvements in sepsis management, mortality still ranges between 20 and 30%. Novel treatment approaches in order to reduce sepsis-related multiorgan failure and death are urgently needed. Robust animal models allow for one or multiple treatment approaches as well as for testing their effect on physiological and molecular parameters. In this article, a simple animal model is presented.
First, general anesthesia is induced in animals either with the use of volatile or by intraperitoneal anesthesia. After placement of an intravenous catheter (tail vein), tracheostomy, and insertion of an intraarterial catheter (tail artery), mechanical ventilation is started. Baseline values of mean arterial blood pressure, arterial blood oxygen saturation, and heart rate are recorded.
The injection of lipopolysaccharides (1 milligram/kilogram body weight) dissolved in phosphate-buffered saline induces a strong and reproducible inflammatory response via the toll-like receptor 4. Fluid corrections as well as the application of norepinephrine are performed based on well-established protocols.
The animal model presented in this article is easy to learn and strongly oriented towards clinical sepsis treatment in an intensive care unit with sedation, mechanical ventilation, continuous blood pressure monitoring, and repetitive blood sampling. Also, the model is reliable, allowing for reproducible data with a limited number of animals in accordance with the 3R (reduce, replace, refine) principles of animal research. While animal experiments in sepsis research cannot easily replaced, repetitive measurements allow for a reduction of animals and keeping septic animals anesthetized diminishes suffering.
Introduction
Sepsis and its more severe form, septic shock, are syndromes on the ground of an infection, resulting in an overshooting inflammatory reaction with the release of cytokines, leading to physiological and biochemical changes with a suppressed immune defense and fatal results1,2. This unbalanced inflammatory reaction results in organ dysfunction and organ failure in various vital organs such as lung, kidney, and liver. With 37%3, sepsis is one of the most common reasons for a patient to be admitted to an intensive care unit (ICU). Mortality of sepsis currently ranges around 20-30%4. Early and effective antibiotic treatment is of utmost importance5. Fluid and vasopressor resuscitation need to be installed early, other than that, treatment is purely supportive6.
Sepsis is defined as a proven or suspected infection with bacteria, fungi, viruses, or parasites, which is accompanied by organ dysfunction. Septic shock criteria are met when a further cardiovascular collapse irresponsive to fluid treatment alone, and a lactate level of more than 2 millimole/liter is present2. Sepsis related organ failure may occur in any organ, but is very common in the cardiovascular system, the brain, the kidney, the liver, and the lung. Most patients suffering from sepsis require endotracheal intubation to secure the patient's airway, to protect from aspiration, and to apply positive end expiratory ventilation with a high fraction of inspired oxygen to prevent or overcome hypoxia. In order to tolerate a tracheal tube and mechanical ventilation, patients usually require sedation.
Endotoxins, such as lipopolysaccharides (LPS) as a component of the membrane of gram negative bacteria induce a strong inflammatory reaction via the toll-like receptor (TLR) 47. Activation of a defined pathway ensures a stable inflammatory reaction. Cytokines like cytokine induced neutrophil chemoattractant protein 1 (CINC-1), monocyte chemoattractant protein 1 (MCP-1), and interleukin 6 (IL-6) are known as prognostic factors for severity and outcome in this model8. Intravenous LPS application has been successfully used to study various aspects of sepsis in rats8,9.
Treatment of sepsis is still a challenge, particularly due to the lack of predictive animal models. If endotoxemia with activation of systemic inflammation is an adequate model for the development of pharmacological therapies is debatable. However, with the well-known LPS-induced TLR 4 pathway important knowledge can be gained.
Protocol
All experiments presented in this protocol were approved by the Veterinary Authorities of the Canton Zurich, Switzerland (approval numbers 134/2014 and ZH088/19). Moreover, all steps performed in this experiment were in accordance with the Guidelines on Experiments with Animals by the Swiss Academy of Medial Sciences (SAMS) and Guidelines of the Federation of European Laboratory Animal Science Associations (FELASA).
1. Anesthesia induction and animal monitoring
- Keep male Wistar rats with a weight of 250-300 gram (g) in ventilated cages under pathogen-free conditions. Provide a 12-12-hour light/dark cycle at an ambient temperature of 22 ± 1 °C, and free access to food and water.
- Induce general anesthesia either by volatile induction with isoflurane (concentration of 3-5%) in an anesthesia induction box for 30 seconds (Figure 1A) or alternatively, induce anesthesia with a single-shot injection of ketamine/xylazine (10/1 milligram (mg) per 100 g body weight).
- Transfer the animal to a working place and lay the animal on a heating-mat throughout the entire experiment. Keep the body-temperature between 36.5 and 37 °C.
- Use a nosecone to provide oxygen (600 mL/minute). Add isoflurane 2-3% if volatile anesthesia was chosen for anesthesia maintenance. Make sure that the animal is spontaneously breathing.
- Confirm the level of anesthesia by the absence of the toe-pinch reflex prior to the installation of tracheostomy and arterial and venous catheters.
- Verify a sufficient oxygenation by peripheral oxygen saturation monitoring (normal oxygen saturation 98 – 100%).
- Use an ointment (Vitamin A ointment) to protect the eyes.
- Prepare sterile surgical instruments and catheters on a side table as displayed in Figure 1B.
- Additionally, prepare pressure and oxygen saturation monitoring as displayed in Figure 1C.
2. Intravenous access
- Apply a tourniquet at the rat's proximal tail to facilitate venous access (Figure 2A).
- Disinfect the tail 3 times with alcohol.
- Induce a G26 intravenous catheter into one of the two lateral tail veins.
NOTE: From our experience it is easier to place the intravenous access at the distal part of the rat's tail, because the vein here is located closer to the skin. In addition, in case of a failed cannulation, there is enough space to move proximally. - Strictly avoid air injection.
- Untie the tourniquet after placing the intravenous catheter.
- Fix the intravenous catheter in place with adhesive tape (Figure 2B).
- Connect syringe-pumps to the intravenous access for continuous fluid and drug application.
- Use 3-way stopcocks for bolus fluid, drug application, and venous blood sampling.
3. Tracheostomy
- Shave the animal's anterior neck-area.
- Disinfect the shaved skin 3 times with providone-iodine solution.
- Perform a circa 2 cm longitudinal incision using a scalpel (with a blade number 10).
- Retract the skin with 2-0 silk sutures.
- Bluntly prepare the larynx and the trachea with surgical scissors (Figure 3A).
- Make sure to open the trachea with surgical micro scissors at the 3-5th tracheal clasp.
- Insert a sterile tracheal cannula into the trachea. Be careful, do not insert the cannula too deeply in order to avoid unilateral ventilation.
- Fix the cannula in place using a 2-0 silk suture.
- Connect the cannula to a ventilator for pressure or volume-controlled ventilation (Figure 3B).
4. Arterial access
- Disinfect the rat tail 3 times with povidone-iodine solution.
- Cut the skin using a scalpel (with a blade number 10) circa 1 cm longitudinally at the ventral side.
- Take care, do not cut too deeply to avoid an injury of the tail artery.
- Use a surgical microscope to expose the artery carefully. Cut the fascia surrounding the artery with surgical micro scissors.
- Ligate the distal part of the artery using a 6-0 silk suture.
- Prepare a proximal 6-0 silk suture but do not tighten the silk (Figure 4A).
- Introduce a G-26 catheter into the artery between the distal and proximal silk suture.
- Once the catheter is in the artery, tighten the proximal silk suture and fix the catheter in place (Figure 4B).
- Connect the catheter to a pressure transducer to provide continuous arterial pressure measurement (normal mean arterial pressure: 60 – 100 mmHg) (Figure 4C).
- Additionally, place a 3-way stopcock between the catheter connected to the pressure transducer and the G-26 catheter for arterial blood sampling.
5. Baseline measurement, sepsis induction and follow-up measurements
- After the animal reached a steady state, inject the LPS.
- Collect blood samples when a steady state is reached (usually after 15-30 minutes).
- Replace fluid loss from blood samples by Ringer's solution in a ratio of 1:4.
- To induce sepsis, inject the LPS as a bolus or as a continuous LPS application.
- For the bolus application, inject 1 mg of LPS/kilogram body weight (kg) dissolved in phosphate buffered saline (PBS) at a concentration of 1 mg/mL.
- For continuous application, inject 300 µg of LPS/kg/hour throughout the entire experiment using a syringe pump (stock solution of LPS: 1 mg/mL in PBS).
- Avoid air-injection at all times in order to prevent air embolism.
- Define fluid replacement protocols, vasoconstrictor application protocols, and abortion criteria (for example hypotension defined as a mean arterial blood pressure below 50 mmHg for more than 30 minutes despite fluid replacement) before setting up the experiment.
NOTE: We suggest a continuous infusion of Ringer's solution at a rate of 10 mL/kg/hour. - Subtract any continuous administration of fluids (e.g., for continuous LPS application) from the amount infused so that the results are comparable with those of the control groups.
NOTE: At the end of the experiment, and prior to harvesting any organs such as liver, kidney or spleen for further analyses such as histological or biochemical examination animals can be euthanized by an incision of the inferior cava vein. The recommended method of euthanasia is to bring the animals to a surgical plane of anesthesia prior to incision of the inferior vena cava and injection of ice-cold saline into the left heart, especially if inflammatory markers in organs are to be assessed. Ensure to comply with the legal requirements and local guidelines. To verify sepsis-related organ failure, pro-apoptosis marker like caspase-3 may be analyzed as well as α1-microglobuline to verify tubular damage in the kidneys. The organ specific analysis of markers like CINC-1, MCP-1 and IL-6 may also provide information about the organ specific inflammatory response.
Representative Results
The system presented allows for endotoxemia with hemodynamically stable animals as reported previously9. While the mean arterial pressure remains stable in animals with, and without LPS stimulation LPS treated animal develop characteristics of sepsis such as a negative base excess and a strong inflammatory reaction measured by plasma cytokines (6 hours after application) such as CINC-1 (867 ng/mL), MCP-1 (5027 ng/mL), and IL-6 (867 ng/mL)8, Figure 5.
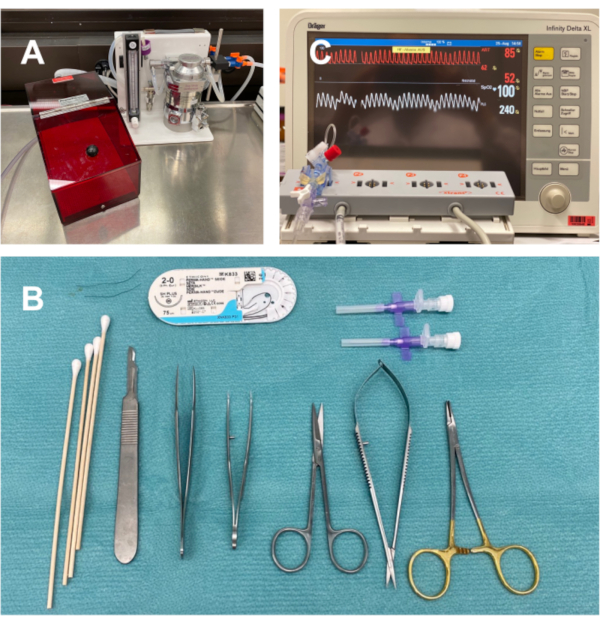
Figure 1: Preparation of equipment: Anesthesia induction box and nosecone for anesthesia/oxygen application (A). Sterile material to be prepared prior surgery: 26G intravenous catheters, a scalpel with a blade number 10, curved forceps, straight forceps, 1 needle-holder, 2-0 and 6-0 silk ties, q-tips, surgical scisors, surgical microscisors (B). Monitoring equipment: Anesthesia monitoring with pressure transducer and a saturation of peripheral oxygenation (SpO2) sensor for continuous monitoring (C). Please click here to view a larger version of this figure.
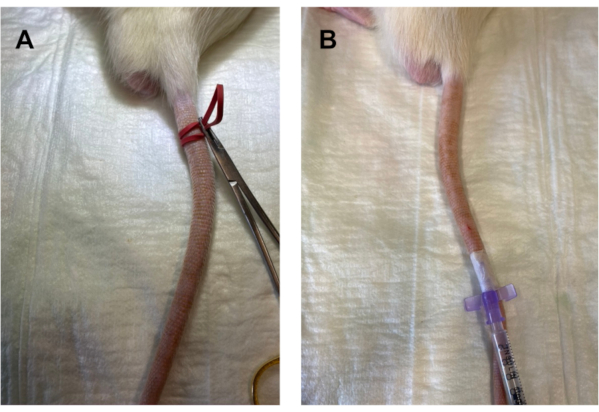
Figure 2: Venous access: A tourniquet is applied to the proximal rat's tail (A). The venous access should be introduced at the distal part of the tail and fixed in place (B). Air embolism should be strictly avoided. Please click here to view a larger version of this figure.
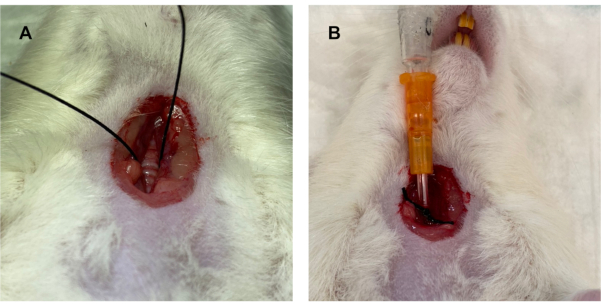
Figure 3: Tracheostomy: The larynx and trachea are bluntly prepared using surgical scissors and exposed using 2-0 silk sutures (A). After opening the trachea using surgical micro scissors at the 3-5th tracheal clasp, a tracheal cannula is introduced, fixed in placed, and connected to a ventilator (B) Please click here to view a larger version of this figure.
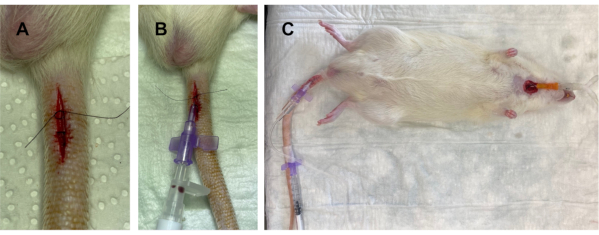
Figure 4: Arterial access: After surgical exposure of the tail artery using a scalpel and surgical micro scissors, a distal silk 6-0 ligature is tightened, and a proximal ligature is prepared (A). After insertion of the G-26 catheter into the artery, it is fixed in place (B). The arterial catheter allows for repetitive blood sampling as well as for continuous blood pressure monitoring (C). Please click here to view a larger version of this figure.
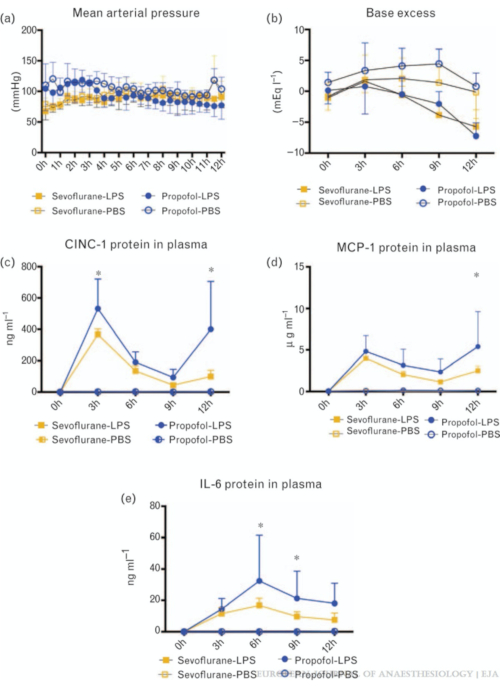
Figure 5: Representative results: While animals remain hemodynamically stable in the LPS as well as in the sham-group (A), they develop characteristics of endotoxemia such as a negative base excess (B) and increased inflammatory mediators such as cytokine induced neutrophil chemoattractant protein 1 (CINC-1) (C), monocyte chemoattractant protein 1 (MCP-1) (D), and interleukin 6 (IL-6) (E). The figure is reproduced with permission from Wolters Kluwer Health Inc., Beck-Schimmer et al, Eur J Anaesthesiol 2017; 34:764-7759. Please click here to view a larger version of this figure.
Discussion
The protocol described here allows for a highly reproducible, yet simple to learn sepsis model, which can be adapted according the research question. Essential in vivo data referring to organ function such as heart rate, blood pressure, and peripheral arterial oxygen saturation may be collected continuously, and blood sampling may be performed repetitively throughout the experiment. In addition, modifications with regard to fluid replacement protocols and vasopressor support can be installed. Given the hemodynamic stability of the animals, experiments can be carried out over several hours, as reported previously8.
It has to be pointed out, that an appropriate sepsis-model has to be chosen in order to answer a specific research question10,11. All sepsis models have their advantages, but also their drawbacks. In the current article, an endotoxemia model is presented, which induces a strong, but sterile inflammation. Key characteristics of sepsis, such as the development of a strong inflammatory response12, endothelial dysfunction and damage13 and multi-organ failure14 are present. Therefore, the model presented is in accordance with the previously published definition of sepsis models in animals by the "International Expert Consensus for Pre-Clinical Sepsis Studies"15. Other key elements may be different than in bacterial sepsis. The LPS bolus application, for example, induces a hypodynamic cardiovascular response16, which does not correspond to the hyperdynamic response observed in human sepsis. The latter, however, may be induced by a continuous LPS infusion as also suggested in the current article16. It has to be considered, that LPS only represents one toxin and may be over-simplified for certain research questions – on the other hand, simplification increases reproducibility of the data. Another characteristic of endotoxemia models is a different cytokine response in comparison to bacterial models – endotoxemia induces higher, yet shorter lasting cytokine elevations10. Although, the model enables repetitive measurements over several hours, the tracheostomy is not ideal for survival experiments. In case of survival experiments, tracheal intubation or spontaneous breathing via a mask may be preferred.
Three fundamentally different classes of sepsis models are currently applied in laboratory sepsis research: toxemia models (e.g., LPS), bacterial infection models (e.g., intravenous Escherichia coli), and host barrier disruption models (e.g., cecal ligation and puncture, CLP)17. Even if toxemia models with LPS were proposed as an inappropriate model for a replication of human sepsis15, it has to be emphasized that characteristics of these fundamental classes of sepsis models have been described in detail8,12,13,14 and been critically reviewed in a recent article17.
There is no final answer, of what humane animal experiments are, but the most common sense is the 3R principle, by their definition, animal experiments should be reduced, replaced, and refined18. While in sepsis research replacement of animal experiments is difficult, repetitive blood sampling and continuous measurements of vital data may reduce the number of animals necessary. Moreover, keeping septic animals anesthetized refines the experimental setup as animal suffering is diminished.
In summary, we present a well-characterized and reproducible model of endotoxemia, a setting similar to that of an intensive care unit with the possibility of generating a high data density, and at the same time limiting the animal burden. In addition, this model can be easily modified depending on the research question needs to be answered.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors would like to thank Beatrice Beck-Schimmer (MD) and Erik Schadde (MD) for their critical examination and their valuable contribution for this manuscript.
Materials
| 2-0 silk sutures | Ethicon, Sommerville, NJ | K833 | Standard surgical |
| 26 intravenous catheter | Becton Dickinson, Franklin Lakes, NJ | 391349 | Standard anesthesia equipment |
| 6-0 LOOK black braided silk | Surgical Specalities Corporation, Wyomissing, PA | SP114 | Standard surgical |
| Alaris Syringe Pump | Bencton Dickinson | ||
| Betadine | Mundipharma, Basel, Switzerland | 7.68034E+12 | GTIN-number |
| Curved fine tips microforceps | World precision instruments (WPI), Sarasota, FL | 504513 | Facilitates vascular preparation |
| Fine tips microforceps | World precision instruments (WPI), Sarasota, FL | 501976 | Tips need to be polished regularly |
| Infinity Delta XL Anesthesia monitoring | Draeger, Lübeck, Germany | ||
| Isoflurane, 250 mL bottles | Attane, Piramal, Mumbai, India | LDNI 22098 | Standard vet. equipment |
| Ketamine (Ketalar) | Pfitzer, New York, NY | ||
| Lipopolysaccharide (LPS) from Escherichia coli, serotype 055:B5 | Sigma, Buchs, Switzerland | ||
| Q-tips small | Carl Roth GmbH, Karlsruhe, Germany | EH11.1 | Standard surgical |
| Ringerfundin | Bbraun, Melsungen, Germany | ||
| Tec-3 Isofluorane Vaporizer | Ohmeda, GE-Healthcare, Chicago, IL | not available anymore | Standard vet. equipment |
| Xylazine (Xylazin Streuli) | Streuli AG, Uznach, Switzerland |
References
- Hotchkiss, R. S., Karl, I. E. The pathophysiology and treatment of sepsis. New England Journal of Medicine. 348 (2), 138-150 (2003).
- Singer, M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Journal of the American Medical Association. 315 (8), 801-810 (2016).
- Vincent, J. L., et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respiratory Medicine. 2 (5), 380-386 (2014).
- Fleischmann, C., et al. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. American Journal of Respiratory and Critical Care Medicine. 193 (3), 259-272 (2016).
- Kumar, A., et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Critical Care Medicine. 34 (6), 1589-1596 (2006).
- Gotts, J. E., Matthay, M. A. Sepsis: pathophysiology and clinical management. British Medical Journal. 353, (2016).
- Akira, S., Takeda, K. Toll-like receptor signalling. Nature Reviews Immunology. 4 (7), 499-511 (2004).
- Urner, M., et al. Insight into the beneficial immunomodulatory mechanism of the sevoflurane metabolite hexafluoro-2-propanol in a rat model of endotoxaemia. Clinical and Experimental Immunology. 181 (3), 468-479 (2015).
- Beck-Schimmer, B., et al. Which Anesthesia Regimen Is Best to Reduce Morbidity and Mortality in Lung Surgery?: A Multicenter Randomized Controlled Trial. Anesthesiology. 125 (2), 313-321 (2016).
- Deitch, E. A. Animal models of sepsis and shock: a review and lessons learned. Shock. 9 (1), 1-11 (1998).
- Buras, J. A., Holzmann, B., Sitkovsky, M. Animal models of sepsis: setting the stage. Nature Reviews Drug Discovery. 4 (10), 854-865 (2005).
- Perretti, M., Duncan, G. S., Flower, R. J., Peers, S. H. Serum corticosterone, interleukin-1 and tumour necrosis factor in rat experimental endotoxaemia: comparison between Lewis and Wistar strains. British Journal of Pharmacology. 110 (2), 868-874 (1993).
- Marechal, X., et al. Endothelial glycocalyx damage during endotoxemia coincides with microcirculatory dysfunction and vascular oxidative stress. Shock. 29 (5), 572-576 (2008).
- Thiemermann, C., Ruetten, H., Wu, C. C., Vane, J. R. The multiple organ dysfunction syndrome caused by endotoxin in the rat: attenuation of liver dysfunction by inhibitors of nitric oxide synthase. British Journal of Pharmacology. 116 (7), 2845-2851 (1995).
- Osuchowski, M. F., et al. Minimum quality threshold in pre-clinical sepsis studies (MQTiPSS): an international expert consensus initiative for improvement of animal modeling in sepsis. Intensive Care Medicine Experimental. 6 (1), 26 (2018).
- Fink, M. P., Heard, S. O. Laboratory models of sepsis and septic shock. Journal of Surgical Research. 49 (2), 186-196 (1990).
- Buras, J. A., Holzmann, B., Sitkovsky, M. Animal models of sepsis: Setting the stage. Nature Reviews Drug Discovery. 4 (10), 854-865 (2005).
- Balls, M. The principles of humane experimental technique: timeless insights and unheeded warnings. Altex-Alternatives to Animal Experimentation. 27 (2), 144-148 (2010).
