The enrolled patient was a 60-year-old woman without any systematic diseases (Figure 1A–D, F). After CBCT scanning, the alveolar ridge in the anterior maxilla was less than 2.9 mm, while the residual bone height in the posterior maxilla region was less than 2.4 mm (Figure 1E, G and Table 1). The width and thickness of the zygomatic bone were approximately 22.4-23.6 mm and 6.1-8.0 mm (Figure 2, Table 3), respectively. According to the Zygoma Anatomy-Guided Approach, the entrance of the anterior ZI was at the level of the canine region, and the posterior ZI was in the second premolar (Figure 3E). The distance between the margin of the anterior ZI and the orbit was 5.2 mm on the right and 3.6 mm on the left, while the distance between the margin of the posterior ZI and the pterygopalatine fossa was 2.9 mm on the right and 4.3 mm on the left (Figure 3F–K).
The surgery was performed using the navigation system (Figure 4A–G). After surgery, the patient received a temporary restoration within 3 days, which addressed both the aesthetic and pronunciation issues (Figure 5C–G). Postoperative CBCT scanning and image integration showed that the errors of the entrance from the left posterior ZI to the left anterior ZI, then to the right anterior ZI, and last to the right posterior ZI were 1.25 mm, 1.35 mm, 1.35 mm, and 1.85 mm, respectively. The errors of the target from the left posterior ZI to the right posterior ZI were 2.25 mm, 1.55 mm, 2.40 mm, and 1.20 mm, respectively. The errors of the ZI angle were 3.50°, 3.59°, 3.20°, and 2.15°, respectively (Figure 5H–I, Table 4).
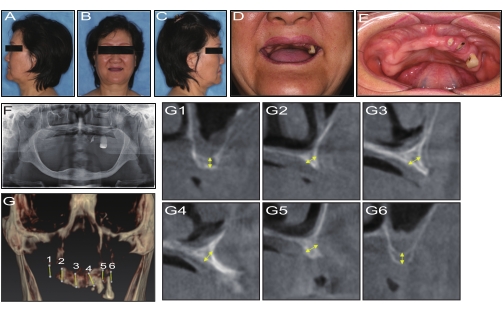
Figure 1: Preoperative examination. (A,C) Preoperative profile view. (B) Preoperative frontal image. (D) Frontal image of the smile line. (E) Intraoral view of the maxilla. (F) Preoperative panoramic radiograph. (G1–6) CBCT curve section. Please click here to view a larger version of this figure.
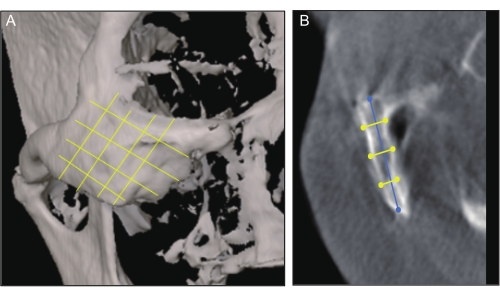
Figure 2: CT measurement. (A) Skull frontal view showing the zygoma divided into superior, middle, and inferior parts by the cross line. (B) Longitudinal tomography showing the measurements of the zygomatic thickness (yellow line) and length (blue line). Please click here to view a larger version of this figure.
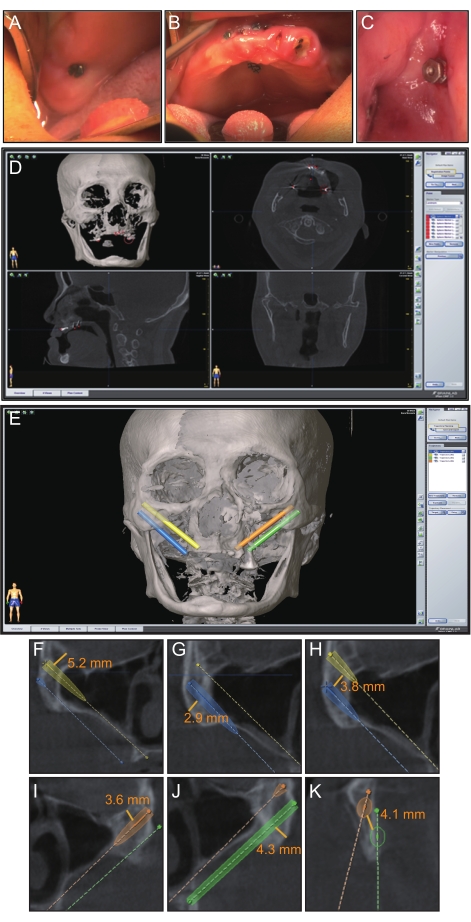
Figure 3: Preoperative planning. (A–C) Eight miniscrews were dispersedly implanted in the remaining maxilla to be registered. (D) Preoperative registration point settings on the navigation software. (E) Preoperative implant planning on the navigation software. (F–K) Distances for ZI planning. Please click here to view a larger version of this figure.
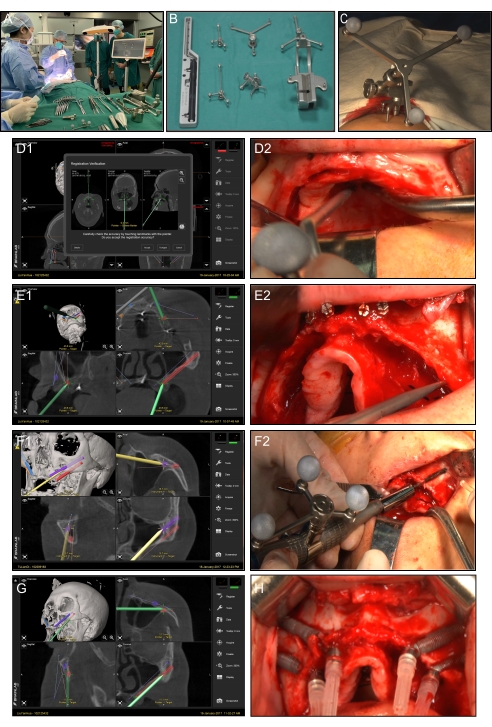
Figure 4: Navigation surgery. (A) Navigation surgery scene. (B) Navigation surgical tools. (C) Cephal bracket mounted to the patient's head for the purpose of tracking. (D1) Screen view of the navigation probe registration application in the sagittal coronal axial. (D2) Intraoral view of the navigation probe application. (E1) Screen view of the entry point location procedure using the navigation probe. (E2) Intraoral view of the procedure using the navigation probe. (F1,F2) Constant visualization of the drilling trajectory displayed on the screen in real-time. The entire procedure from the entry point to the exit point. (G) Screen view of the ZI position verification using the navigation probe. (H) Accomplishment of ZI placement. Please click here to view a larger version of this figure.
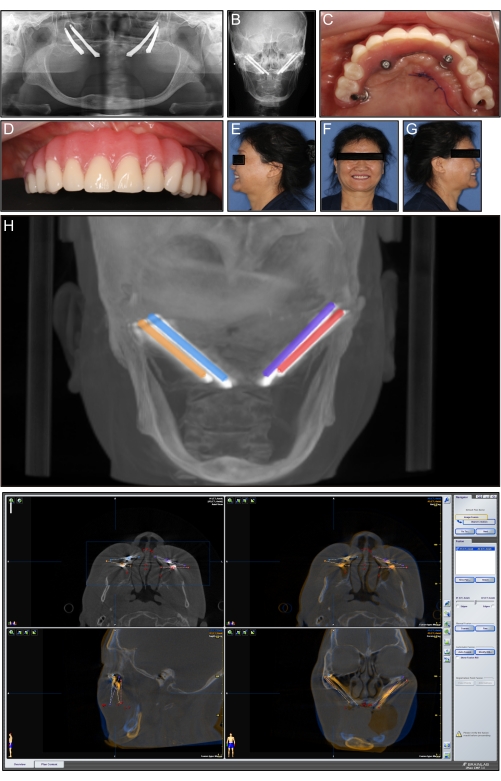
Figure 5: Postoperative view and image infusion. (A) Postoperative panoramic radiograph. (B) Postoperative frontal cephalometrics. (C) Intraoral view of the immediate temporary restoration. (D) Anterior view of the immediate temporary restoration. (E) Postoperative profile view after the immediate temporary restoration. (F) Frontal image after the immediate temporary restoration. (G) Postoperative profile view after the immediate temporary restoration. (H) Preoperative image integrated with the postoperative image, and measurement of the planned-placed deviations of implants. (I) Postoperative CBCT image integration observed in sagittal, coronal, and axial view. Please click here to view a larger version of this figure.
| Inclusion criteria | Exclusion criteria |
| 1. Completely edentulous maxilla or be going to be edentulous maxilla | 1. Sufficient bone for conventional implant treatment |
| 2. Severe atrophy of the maxilla | 2. Bone graft was considered more appropriate |
| 3. Age range from 18-80 | 3. Untreated maxillary sinusitis |
| 4. Insufficient width for anterior maxilla to place regular implants of at least 3.75 mm | 4. Local or systemic contraindications for oral surgery |
| 5. Maxillary posterior bone height ranging from 1 to 3 mm in the premolar and molar regions | 5. A medication history of bisphosphonates |
| 6. The bone thickness for placing the apex of the ZI was at least 5.75 mm |
Table 1: Patient inclusion and exclusion criteria.
| Anterior region width (mm) | Pre-molar region width (mm) | Molar region height (mm) | |
| Left | 2.8 | 2.5 | 2.4 |
| Right | 2.9 | 2.9 | 2.2 |
Table 2: Differences in alveolar bone thickness at points on the anterior region, and residual alveolar bone height at points on the premolar region and molar regions.
| Zygomatic bone thickness (mm) | Zygomatic bone width (mm) | |||||
| Superior | Middle | Inferior | Superior | Middle | Inferior | |
| Left | 7.4 | 5.3 | 7.8 | 23 | 23.6 | 24.1 |
| Right | 8 | 6.1 | 5.7 | 22.4 | 23.1 | 25.9 |
Table 3: Differences in zygomatic thicknesses at points on the superior, middle, and inferior areas.
| Starting position error (mm) | Teminal position error (mm) | Angular deviation (°) | |
| Distal of the left ZI | 1.25 | 2.25 | 3.5 |
| Mesial of the left ZI | 1.35 | 1.55 | 3.95 |
| Mesial of the right ZI | 1.35 | 2.4 | 3.2 |
| Distal of the right ZI | 1.85 | 1.2 | 2.15 |
Table 4: Resulting deviation of four zygomatic implants.
