Physiological parameters
Mice recovered from this unilateral renal IRI surgery uneventfully; appeared active and alert; and showed normal eating, drinking, and behavior by the following day. Some mice may have post-IRI body weight loss, although it is usually less than 10% of the initial body weight (Figure 2). Greater body weight losses (˃10%) can be detrimental, and those animals should be removed from the study. Sham-operated mice did not show body weight changes post-surgery (measured 24 h after surgery). Most mice recovered their initial body weight between days 4 and 7 post-surgery (see IRI 7-day group, Figure 2). Renal function can be assessed using traditional markers such as blood urea nitrogen (BUN) and creatinine. Additionally, electrolyte levels in serum (sodium, potassium, and chloride) and an automated differential blood count were included in the analysis.
Histopathological changes
Assessment of histopathological findings was done using 4% paraformaldehyde-fixed, paraffin-embedded whole mid-sagittal sections of the kidney stained with hematoxylin/eosin (HE), periodic acid Schiff, and Masson's trichrome stains. The most evident changes produced by this unilateral renal IRI model can be seen at the cortico-medullary junction, specifically in the proximal tubules, thick ascending limbs of Henle's loop, and distal convoluted tubules, as well as in the tubular interstitium (see the legend for Figure 3). Microscopic images showing the most characteristic lesions following IRI in the kidney can be seen in Figure 3. A list of the sequential histopathological findings is provided in Table 1.
A tubular injury scoring system was developed to categorize the damage over time (Figure 4). In this, five defined alterations were assessed by three different evaluators: 1) tubular epithelial attenuation; 2) brush border loss; 3) tubular necrosis; 4) luminal obstruction; and 5) presence of proteinaceous cast. An assignment of "1" indicates that the alteration is present, "0" that it is absent.
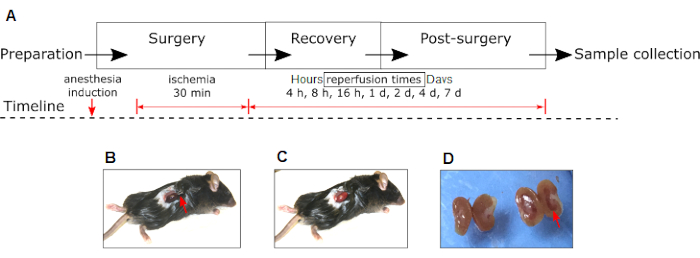
Figure 1: Experimental renal IRI model in mouse. (A) Phases of experiments and interventions (anesthesia induction, ischemia, and reperfusion) are shown. Please note the changes in the color of the right kidney to dark red during ischemia (B) to pink during reperfusion (C). (D) Macroscopic appearance of the IRI right kidney (red arrow) compared to the contralateral non-IRI kidney of the same animal 24 h after surgery. Red arrow in (B) shows the position of the hemostatic clamp. Abbreviation: IRI = Ischemia-reperfusion injury. Please click here to view a larger version of this figure.
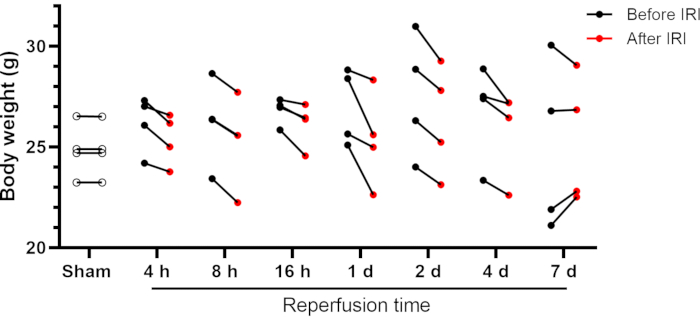
Figure 2: Body weight of mice before and after renal IRI. Individual data are shown. Abbreviations: IRI = Ischemia-reperfusion injury; h = hours; d = days. Please click here to view a larger version of this figure.
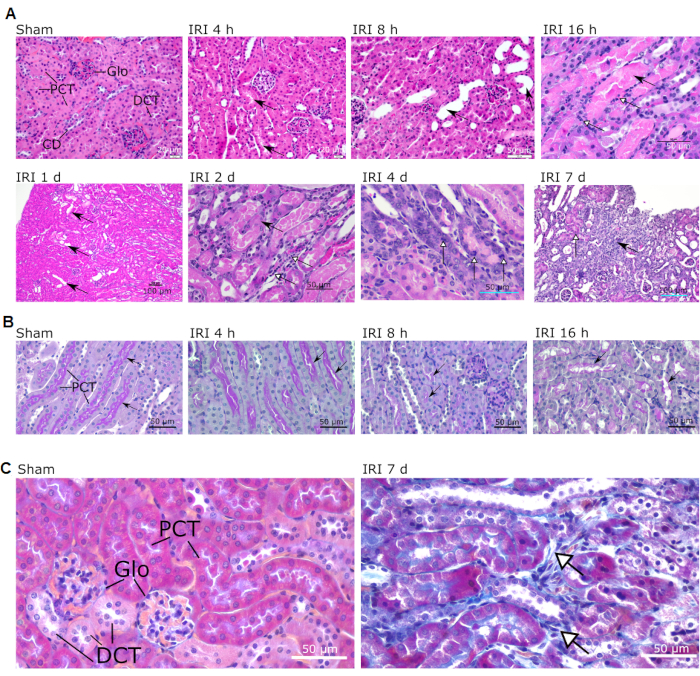
Figure 3: Typical microscopic lesions observed in the cortex and the cortico-medullary junction of IR-operated mice. Sham and different reperfusion times are shown (indicated above each picture). (A) Intact structures are shown in sham (magnification 40x; scale bar = 20 µm). Arrows in IRI 4 h indicate the presence of proteinaceous cast in the tubular lumen (magnification 40x; scale bar = 20 µm). Arrows in IRI 8 h show tubular dilatation (magnification 40x; scale bar = 50 µm). Black arrow in IRI 16 h shows tubular cast in medullary segments; white arrows show areas of cellular necrosis (magnification 40x; scale bar = 50 µm). Black arrows in IRI 1 d indicate tubular dilatation (magnification 10x; scale bar = 100 µm). Black arrow in IRI 2 d shows enlarged cell nuclei; white arrowheads show areas of lymphocyte and macrophage infiltration (magnification 40x; scale bar = 50 µm). White arrowheads in IRI 4 d indicate mitotic tubular cells (magnification 40x; scale bar = 50 µm). Black arrow in IRI 7 d shows an area of focal fibrosis; white arrowhead shows an area of regeneration (magnification 20x; scale bar = 100 µm). (B) PAS staining showing the renal cortex of mice during early reperfusion (4 h, 8 h, and 16 h). Note the progressive attenuation of the brush border (arrows). Magnifications 40x; scale bars = 50 µm (C) Masson trichrome staining of sham and IRI 7 d mice showing areas of interstitial fibrosis (white arrows). Magnification 40x; scale bars = 50 µm. Abbreviations: IRI = Ischemia-reperfusion injury; Glo = glomerulus; PCT = proximal convoluted tubule; DCT = distal convoluted tubule; CD = collecting duct; PAS = periodic acid Schiff; d = day. Please click here to view a larger version of this figure.
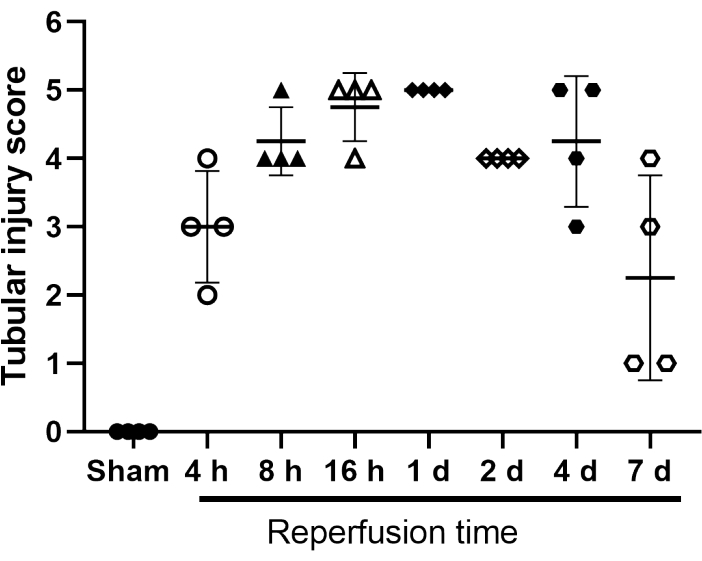
Figure 4: Tubular injury score of sham- and IRI-operated mice. Scoring system scale 1 to 5 for tubular epithelial attenuation; brush border loss; tubular necrosis; luminal obstruction; and presence of proteinaceous cast. An assignment of "1" indicates that the alteration is present, "0" that it is absent. Individual values are shown. Bars represent mean ± SD (n = 4). Abbreviation: IRI = Ischemia-reperfusion injury. Please click here to view a larger version of this figure.
| Time after IRI | Most significant pathological changes |
| 4 h | Tubular obstruction |
| Protein cast in lumen | |
| 8 h | Tubular dilatation |
| Incipient necrosis | |
| Attenuation of epithelium | |
| 16 h | Cellular necrosis |
| Tubular cast | |
| Neutrophil infiltration | |
| 1 day | Necrosis |
| Tubular dilatation | |
| Neutrophil infiltration | |
| 2 days | Tubular dilatation |
| Lymphocyte and macrophage infiltration | |
| Enlarged cell nuclei | |
| 4 days | Prominent mitotic activity in tubule cells |
| 7 days | Focal fibrosis |
| Areas of regeneration |
Table 1: Most significant pathological changes over time. Diagnosed based on microscopic examination of 4-6 animals per group.
