The overall schematic process of performing a 4-color multiplex assay for the detection of 4 endometrial immune cell types is shown in Figure 1. In brief, the protocol for this multiplex immunofluorescence staining required 8 key steps: 1. Slide preparation, 2. Epitope retrieval, 3. Blocking, 4. Primary antibody application, 5. Secondary antibody application, 6. Signal amplification, 7. Removal of antibody, and 8. Counterstain and mount. Image rendering and analysis were then conducted using the Mantra Workstation with the spectral library generated using the inForm Image Analysis software for differentiating the 4 immune cell types in the endometrium sample (Figure 2).
Four endometrial immune cell types can be identified in human endometrium samples using this multiplex staining technique: CD3+ T cells, CD20+ B cells, CD68+ macrophages, and CD56+ uNK cells (Figure 3). However, fluorophore interference must be carefully considered to obtain a clear and useable image. Although this multispectral technology using the Mantra Workstation can support up to 8-plex assays, the application of the 4 fluorophores used in this protocol demonstrated optimal performance without fluorophore interference due to the differences in emission spectra of the fluorophores. In contrast, multiplex staining involving 5-8 fluorophores often requires more attention toward fluorophore interference resulting from emittance from the shared wavelengths.
To overcome this drawback, monoplex staining would be necessary to determine the order of each antibody in the multiplex and identify the expression level and pattern of each immune marker in the endometrium sample. This can help to determine the staining sequence of the markers and their associated TSA fluorophore pairings. Once the monoplex assay has been completed for determining the order of antibodies to be applied, the next step will be to select the fluorophore for detection after multiplex staining. A unique fluorophore must be chosen for every antibody of interest. The number related to each fluorophore would roughly be the fluorescent wavelength emitted during excitation (Table 1 and Table 2). One approach to prevent fluorophore interference is to choose fluorophore pairs with wavelengths as far from each other as possible (especially for co-localizing antibodies). This can help reduce excess spectral overlap and provide a crisp image and more reliable phenotyping. Moreover, the meticulous evaluation by turning lasers on and off from the multiplex composite image in the inForm software can also help recognize the staining patterns to minimize fluorophore saturation (Figure 4).
For image analysis, the number of CD3+ T cells, CD20+ B cells, CD68+ macrophages, CD56+ uNK cells, and stromal cells in the endometrial stroma (CD3−/CD20−/CD68−/ CD56− and DAPI-stained) can be counted automatically using the inForm Tissue Finder Software 14.0 (Figure 5). Each immune cell type density was expressed as a percentage relative to the total number of stromal cells (Figure 5). Similarly, the quantification of the spatial distribution of the endometrial immune cells was based on the X and Y position of every single immune cell obtained from the InForm system (Figure 6). Using the R-language, the level of clustering of different pairs of immune cells based on the AUC can then be distinguished.
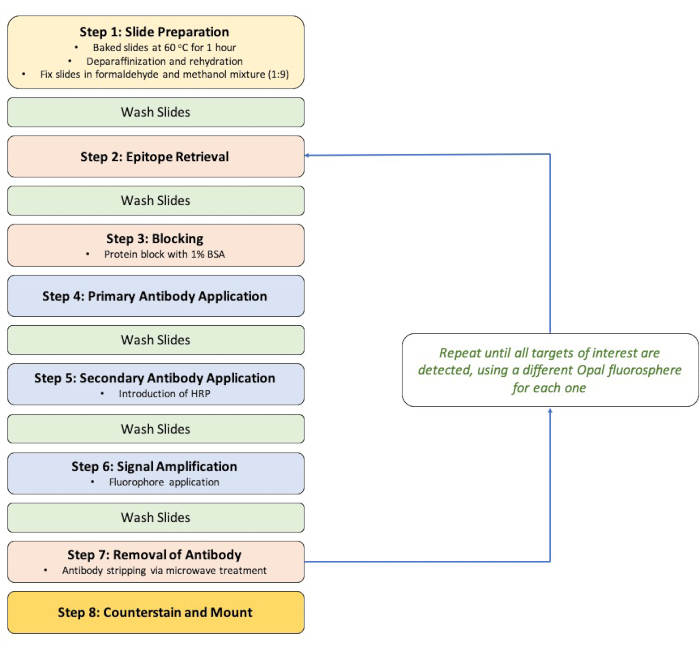
Figure 1: Staining workflow diagram. Abbreviations: BSA = bovine serum albumin; HRP = horseradish peroxidase. Please click here to view a larger version of this figure.
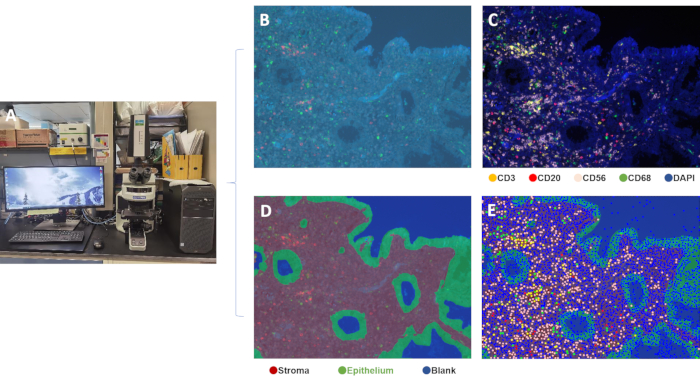
Figure 2: Workstation for image capture and analysis. (A) Mantra Imaging Workstation, (B) unprocessed Spectral image, (C) composite image, (D) tissue segmentation (epithelial and stromal compartments), (E) composite image of endometrium tissue showing four colored markers to identify different cell populations. Please click here to view a larger version of this figure.
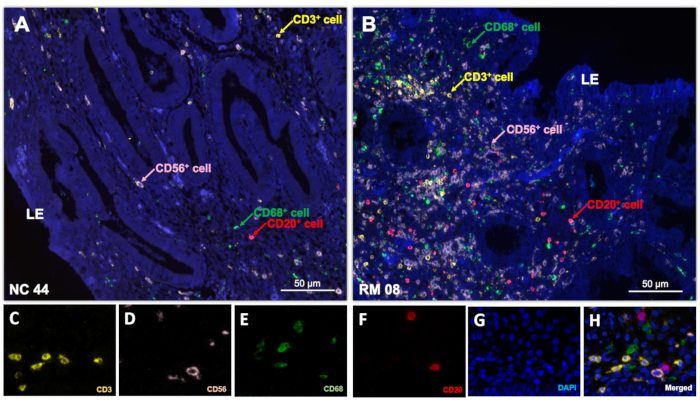
Figure 3: Spectral imaging. Multiplex immunostaining of 4 different immune cell types was performed on the endometrial biopsies from (A) a fertile control woman and (B) a woman with unexplained RM presented as single multispectral imaging. Following the production of a single-stained library, spectral unmixing could reveal imaging of single fluorophores representing (C) CD3, (D) CD56, (E) CD68, (F) CD20, (G) DAPI. A composite image was then created by incorporating all the fluorophores after multispectral imaging (H). Scale bars = 50 µm (A, B). Abbreviations: LE = luminal epithelium; DAPI = 4′,6-diamidino-2-phenylindole; RM = recurrent miscarriage. Please click here to view a larger version of this figure.
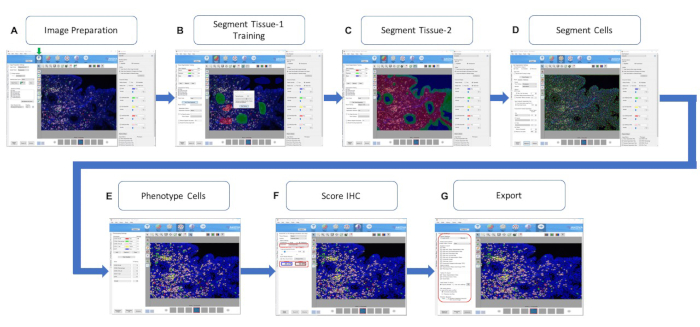
Figure 4: InForm Counts Tool. The inForm software counts tool is activated by selecting the beige box icon (indicated by ↓). (A) Image preparation, (B, C) segmenting tissue for hand-drawn training and automation, (D) segmenting individual cells, (E) phenotyping the cells based on the fluorophore intensity, (F) analysis for fluorophore intensity (the red box showing the number of positive cells in the selected fluorophore intensity), and (G) exporting the results for use (the red box indicates the export options). Abbreviation: IHC = immunohistochemical. Please click here to view a larger version of this figure.
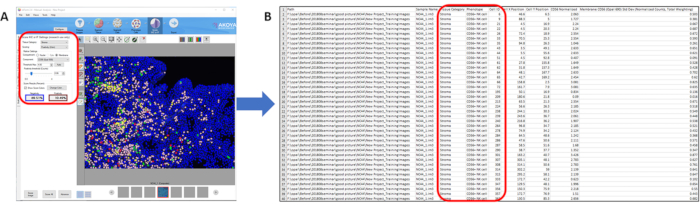
Figure 5: Cell Counting. (A) Phenotyping of the cells for automatic cell counting and (B) output of the positive-stained cells in the segmented region (e.g., stromal) for further comparison and statistical analysis. Please click here to view a larger version of this figure.
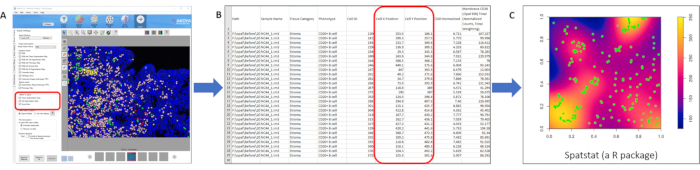
Figure 6: Measurement of spatial density. (A) Automatic detection of the position of positively stained immune cells in the segmented region (e.g., stromal), (B) output display of the coordinate of each positively stained CD20+ immune cell, and (C) determining the spatial density and localization between CD20+ cells and other immune cells in the segmented tissue regions using Spatstat. Please click here to view a larger version of this figure.
| Order | Antibody | Clone | Clonality | Antibody Dilution Factor | Opals | Opal Dilution Factor |
| 1 | CD3 | SP7 | Monoclonal | 1 in 100 | Opal 620 | 0.111111111 |
| 2 | CD20 | L26 | Monoclonal | 1 in 100 | Opal 650 | 0.215277778 |
| 3 | CD68 | SP251 | Monoclonal | 1 in 100 | Opal 520 | 0.111111111 |
| 4 | CD56 | CD564 | Monoclonal | 1 in 100 | Opal 690 | 0.111111111 |
Table 1: List of antibodies, clones, and concentrations used.
| Dye | Excitation maximum (nm) | Emission maximum (nm) | Expected Detection in Filter Set (name) | Expected Color |
| DAPI | 350 | 470 | DAPI | Blue |
| Opal 520 | 494 | 525 | FITC | Green |
| Opal 620 | 588 | 616 | Cy3 and Texas Red | Amber |
| Opal 650 | 627 | 650 | Texas Red and Cy5 | Orange |
| Opal 690 | 676 | 694 | Texas Red and Cy5 | Clear |
Table 2: List of fluorophores with their maximum excitation and emission wavelengths, expected detection in appropriate filter sets, and observable colors.
