The following protocol was approved by Rutgers University Institutional Review Board. All volunteers participating in this study provided written informed consent prior to all testing.
1. Pre-test preparation
- Assess the individual for allergies or sensitivity to mouthpiece or nose clip materials, for oral or facial pain preventing proper seal on the mouthpiece, for an ability to follow directions, and for known sensitivity to the bronchodilating agent that will be used.
- Ensure that the individual dresses comfortably and refrains from exercising or ingesting a heavy meal before testing. Refer to local laboratory policies regarding the use of caffeine, tobacco products, or inhaler before testing.
- Perform FOT first in situations of multiple pulmonary function tests requiring deep breaths.
- Perform testing in a quiet and comfortable environment. Prepare supplies and materials prior to the individual's arrival.
- Provide an adjustable chair without wheels to ensure that the individual's feet are flat against the floor.
- Provide the individual with a disposable anti-bacterial filter and nose clip to be used for testing.
- Adhere to local laboratory procedures for donning personal protective equipment when testing.
2. Verification with impedance test load
- Locate the test load object before testing the individual.
NOTE: Static test loads are manufacturer-supplied objects with known impedance (preferably with resistive, elastic, and inertial components) that are specific to each device. Use a test load with an impedance of approximately 15 hPa·s·L-1, which exceeds the expected Zrs for adults. - Ensure that the test load is factory calibrated (if applicable).
NOTE: Some test loads require annual factory recalibration, so follow the protocol outlined in the device manual.- Consult the manual or contact the manufacturer if the test load for verification is accidentally dropped or visually appears damaged.
- Open the calibration or verification menu within the software.
- Firmly insert the test load device into the FOT device and complete the verification procedure according to the manufacturer's recommendations.
- Review and save the verification results.
NOTE: A successful verification ensures that the measured values match the test load within a tolerance of ≤+10% or ±0.1 hPa·s·L-1. If the verification fails or gives errors, ensure that the test load was properly seated into the FOT device and there is no obstruction in the flow. Consult the manual for troubleshooting tips. - Verify the device with the test load daily, or immediately before testing.
3. Test procedure
- Provide standardized instructions and demonstration for the individual.
- Let the individual know about the approximate duration of a single acquisition and the number of replicates that will be taken (see step 3.2).
- Let the individual know about the sensations that they will experience from the oscillations, e.g., fluttering or vibrations in the chest and mouth.
- Let the individual know that the device will start oscillations after a brief period of observation to regulate breathing.
- Instruct the individual to avoid swallowing during the testing period.
- Instruct the individual to sit upright with the feet flat on the floor and the chin facing up for the duration of the testing period.
- Instruct the individual to create a seal with the lips and teeth on the mouthpiece via a demonstration.
- Instruct the individual to keep the tongue relaxed.
- Instruct the individual to firmly place open palms against cheeks with fingertips near the temple and thumbs following the mandibular line. Instruct the individual to keep the elbows slightly flared in a comfortable position to ensure chest expansion.
- Instruct the individual to maintain regular quiet breathing on the mouthpiece until asked by the technician to stop.
- Perform measurement session
- Adhere to hygiene and infection control standards as described for spirometry15.
- Attach the anti-bacterial filter to the device.
NOTE: Use filters that meet ATS/ERS guidelines with a resistance <1.5 hPa·s·L-1 at a flow rate less than 14 L/s as verified by the manufacturer. - Provide instructions as described in step 3.1 and ensure that the individual is positioned correctly with the nose clip in place and mouth tightly sealed around the mouthpiece of the device.
- After the individual completes several respiratory cycles of stable, passive, and comfortable tidal breathing, ensure that the device automatically begins acquiring data. Alternatively, the technician may trigger data acquisition using the software.
- Instruct the individual to come off the mouthpiece after at least three artifact-free breaths are acquired during a single acquisition.
NOTE: To achieve three artifact-free breaths, a minimum recording duration of 30 s is recommended. Some FOT devices' settings will automatically stop at a pre-defined recording duration and/or achievement of a certain number of breaths (see section 4 for details on identifying artifacts). - Adjust the rest intervals between replicate measurements (approximately 60-90 s) as needed to avoid any physical discomfort.
- Optionally, assess the bronchodilator response.
- Administer salbutamol to the individual in accordance with standard laboratory procedures for aerosol medications (e.g., metered dose inhaler, nebulizer) and wait for 15 min16.
NOTE: If using a metered dose inhaler with a spacer, administer four separate doses of 100 µg. - Repeat the same procedures as before (see step 3.2) to obtain post-bronchodilator replicates.
- Administer salbutamol to the individual in accordance with standard laboratory procedures for aerosol medications (e.g., metered dose inhaler, nebulizer) and wait for 15 min16.
4. Determining acceptable measurements
- Identify artifacts through visual inspection. To do so, monitor the depth (tidal volume; Vt) and rate of breathing (respiratory frequency; fR) in real-time during acquisition to visually ensure stable and quiet breathing patterns from replicate to replicate.
NOTE: For each replicate, the average Vt, fR, or their product (minute ventilation, V̇E) will be displayed within the software. Compare this value between replicates in order to provide individual feedback on the depth and rate of breathing, if necessary. - Inspect the replicate manually to exclude artifacts such as cough, swallowing, leak, or other interruptions to flow and pressure traces that can be viewed in real-time.
- Discard any replicates containing negative resistances.
- Review automatic software detection of artifacts.
NOTE: Manufacturers employ software algorithms for detecting artifacts and excluding whole or partial breaths (i.e., inspiration and expiration). Get familiarized with the algorithms applied and report this when summarizing data from a measurement session. Often, these algorithms involve identifying Rrs, Xrs, and breathing patterns outside of normal physiological ranges as well as outliers when comparing breath-by-breath. - Assess variability
- Acquire at least three acceptable replicates (i.e., those containing ≥3 artifact-free breaths). Calculate the within-session coefficient of variation (CoV) for total Rrs at the lowest frequency (e.g., Rrs at 5 Hz).
NOTE: CoV is calculated using the following formula:

- As the acceptable within-session CoV for adults is ≤10%, obtain additional replicates if the CoV is >10% or proceed to step 5 if CoV is ≤10%.
NOTE: Achieving CoV ≤10% may be difficult in individuals with airway disease.
- Acquire at least three acceptable replicates (i.e., those containing ≥3 artifact-free breaths). Calculate the within-session coefficient of variation (CoV) for total Rrs at the lowest frequency (e.g., Rrs at 5 Hz).
5. Reporting data
- Include the following details when reporting FOT results.
- Include the device name, model, software version, and manufacturer.
- Include input stimulus frequency waveform (e.g., pseudo-random noise, multi-frequency) and associated frequency range.
- Include the details on subjective and automatic quality control procedures used to determine acceptable replicates and the number of artifact-free replicates included.
- Include the repeatability or precision of measurement (CoV) and cut-off.
- Report the mean of the replicate measurements that were free of artifact and provided a CoV ≤10% for FOT parameters.
- Adhere to laboratory standards regarding which FOT parameters to report.
NOTE: While there is currently no consensus on which FOT variables to include, the ERS Technical Standard provides an example of what parameters might be reported as shown in Table 1 for the case example results presented below.
- Adhere to laboratory standards regarding which FOT parameters to report.
- Utilize reference equations from the population being studied using the same FOT device (if available).
NOTE: Many reference equations will assume accurate recording of age, sex, height, and weight14. - Optionally, report both the absolute and relative difference if FOT was performed before and after a bronchodilator. Also, include the dose of salbutamol.
6. Quality control and maintenance
- Employ a quality control program using biological controls (i.e., ≥2 healthy non-smoking individuals) that involves routine testing on a periodic basis.
- Establish a baseline (mean ± SD) through the acquisition of 10-20 artifact-free replicate measurements on different days (acquired within 2 weeks) from each biological control.
- Select a low- (5 Hz) and mid-frequency (20 Hz) parameter for resistance and reactance to follow for quality control. On subsequent routine periodic testing, compare the results to the baseline measures.
NOTE: Refer to recommended guidance for pulmonary function laboratories17 for additional details on how to assess and enact quality assurance standards. The frequency of biological control testing (e.g., weekly, monthly) should reflect the volume of testing in the laboratory.
- Follow the manufacturers' recommendations on regular maintenance such as cleaning, air filter change, software updates, and factory calibration.
First, a case of a healthy adult is presented as a practical example of data acquisition and how the technician selects individual measurements for reporting (Case Example 1). Second, a clinical example is provided of a patient referred for unexplained dyspnea for FOT acquisition before and after a bronchodilator with emphasis on interpretation (Case Example 2). Note that FOT devices from two different manufacturers have been purposefully used in these case examples to illustrate a universal approach. Additional details are provided in the Table of Materials.
Case Example 1
FOT was performed in a healthy 25-year-old Hispanic female (Height: 164 cm, Weight: 84.9 kg). The participant was a never-smoker, denied respiratory symptoms, and had no history of lung disease or other significant past medical history. She had abstained from caffeine (≥8 h) and vigorous exercise (≥24 h). She had a recent spirometric examination that was read as normal without signs of obstruction or restriction: FEV1/FVC: 0.88, FEV1: 3.30 L (98% predicted), and FVC: 3.70 L (97% predicted).
After explaining and demonstrating test procedures, three FOT measurements were obtained with approximately 1-2 min between recordings. Visual inspection and the software's quality control algorithm did not identify any artifacts. Rrs at 5 Hz for the first three measurements was then examined to confirm within-session CoV (individual measurements: 3.06, 3.79, 3.46 hPa·s ·L-1; average: 3.44 hPa·s·L-1, standard Deviation: 0.36 hPa·s L-1, CoV = standard deviation / average = 0.36 / 3.44 = 0.105 * 100 = 10.5%).
Since the CoV of the first three measurements was >10%, additional measurements were necessary. A fourth measurement was obtained (Rrs at 5 Hz = 3.40 hPa·s·L-1) and within-session CoV was recalculated using all measurements (individual measurements: 3.06, 3.79, 3.46, 3.40 hPa·s·L-1; average: 3.43 hPa·s·L-1; standard Deviation: 0.30 hPa·s·L-1; CoV = standard deviation / average = 0.30 / 3.43 = 0.087 * 100 = 8.7%)
Because the within-session CoV criteria were met, average FOT indices were calculated as the average of measurements. These measurements are illustrated in Figure 1 and reported in Table 1. Additionally, to facilitate comparison to expected values, Table 2 presents predicted values across all FOT indices (where predicted values are available), lower limits of normal (LLN), upper limits of normal (ULN), % of predicted and Z-scores using standard reference equations that consider age, sex, and weight14.
Case Example 2
A 48-year-old Caucasian male (Height: 185 cm, Weight: 89 kg) was referred to our center for evaluation of chronic cough and exertional dyspnea without obvious cause (e.g., medication, respiratory or cardiovascular disease, or mental health comorbidity). He was a lifetime never-smoker but endorsed exposure to vapors, gases, dust, and fumes during a 7-month military deployment to Iraq. Complete pulmonary function testing was performed (i.e., body plethysmography, bronchodilator spirometry, and lung diffusing capacity for carbon monoxide) and all results were within normal limits. FOT was performed before and 15 min after administration of bronchodilator (4 puffs of 100 µg salbutamol via metered-dose inhaler with spacer) (Figure 2). The individual trial data and mean values are presented in Table 3 pre- and post-bronchodilator administration; as each trial was technically acceptable, the pre- and post-bronchodilator measurements, as well as their absolute and relative difference, are reported in Table 4. In addition, predicted values, % of predicted, LLN, and ULN are also reported using standard reference equations that consider age, sex, and weight14.
We delimited variables reported in Table 3 and Table 4 to simplify the illustration of two concepts: 1) determining abnormal versus normal responses, and 2) bronchodilator reversibility. For Rrs measurements, values that exceed the ULN (i.e., elevated resistance) are considered abnormal. Here, pre-bronchodilator Rrs at 4 Hz (3.32 hPa·s·L-1) exceeds the ULN (2.59 hPa·s·L-1) and is 155% of the predicted value ([3.32 / 2.14] * 100 = 155.14). Following bronchodilator administration, Rrs at 4 Hz was reduced by 45.78% exceeding the 95th percentile reported by Oostveen et al.14 (i.e., -32% for Rrs at 4 Hz). This response would indicate a positive bronchodilator response in resistance. Additionally, the post-bronchodilator observed value is normalized (i.e., became representative of what is considered a normal value) and is 84.1% of the predicted value ([1.80 / 2.14] * 100 = 84.11).
Xrs at 4 Hz is interpreted differently as observed values are negative. Therefore, abnormal values are those that exceed the LLN (i.e., more negative reactance). Here, the individual had a pre-bronchodilator (-0.98 hPa·s·L-1) and post-bronchodilator (-0.83 hPa·s·L-1) values that are above the LLN (-1.11 hPa·s·L-1). The difference in pre- versus post-bronchodilator was approximately 15%, which is below the 95th percentile reported by Oostveen et al.14 (i.e., +33.8% in Xrs at 4 Hz). Therefore, all Xrs values are considered normal.
Reactance area (or AX) is the integrated area of low-frequency reactance and, therefore, is a positive value. Abnormal AX values are those that exceed the ULN, reflecting more negative reactance. Like Xrs at 4 Hz, pre-bronchodilator AX (2.77 hPa·s·L-1) and post-bronchodilator AX (1.23 hPa·s·L-1) are both below the ULN. Although there was a reduction of -55% from pre- to post-bronchodilator value, this falls below the 95th percentile reported by Oostveen et al.14 (i.e., -56.0% for AX at 4 Hz). Taken together, AX is considered normal as well.
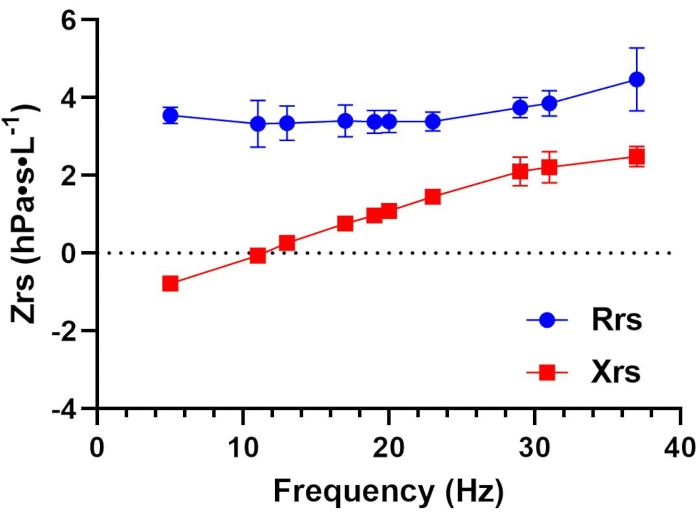
Figure 1: Respiratory resistance (Rrs) and reactance (Xrs) as a function of oscillation frequency (Hz) in a healthy adult. Mean ± SD of all replicates are plotted for Rrs (blue circles) and Xrs (red squares) at each measured frequency. Each data point represents total or whole-breath measurements. Data were collected using a device that employs a pseudorandom, relative primes signal type in the 5-37 Hz range. Please see the Table of Materials for additional details regarding this device. Please click here to view a larger version of this figure.
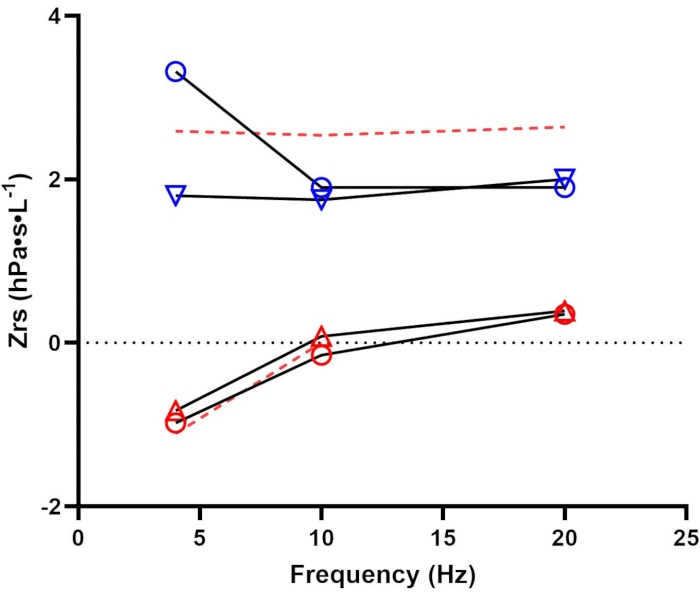
Figure 2: Pre- and post-bronchodilator assessment. Respiratory resistance (Rrs; blue) and reactance (Xrs; red) before (open circles) and after (open triangles) bronchodilator administration. Dashed red lines represent the upper and lower limits of normal for Rrs and Xrs, respectively14. Data were collected using a device that employs a pseudorandom signal type in the 4-48 Hz range. Please see the Table of Materials for additional details regarding this device. Please click here to view a larger version of this figure.
| Variable | T1 | T2 | T3 | T4 | Avg | SD |
| Rrs5 | 3.06 | 3.79 | 3.46 | 3.40 | 3.43 | 0.30 |
| Rrs5 (insp) | 3.30 | 3.45 | 3.34 | 3.64 | 3.43 | 0.15 |
| Rrs11 | 2.77 | 4.02 | 3.08 | 2.89 | 3.19 | 0.57 |
| Rrs19 | 2.92 | 3.71 | 3.30 | 3.13 | 3.27 | 0.33 |
| Rrs5-19 | 0.14 | 0.08 | 0.15 | 0.26 | 0.16 | 0.08 |
| Xrs5 | -0.90 | -0.76 | -0.69 | -0.90 | -0.81 | 0.11 |
| Xrs5 (insp) | -1.44 | -0.91 | -0.86 | -1.08 | -1.07 | 0.26 |
| Xrs5 (exp) | -0.63 | -0.46 | -0.55 | -0.77 | -0.60 | 0.13 |
| Delta Xrs5 | -0.81 | -0.45 | -0.31 | -0.31 | -0.47 | 0.24 |
| Xrs11 | -0.04 | -0.09 | 0.00 | -0.09 | -0.06 | 0.04 |
| Xrs19 | 0.92 | 0.86 | 1.12 | 0.94 | 0.96 | 0.11 |
| AX | 2.83 | 2.57 | 2.05 | 2.98 | 2.61 | 0.41 |
| Fres | 11.27 | 11.62 | 10.99 | 11.57 | 11.36 | 0.29 |
| Vt | 0.90 | 0.98 | 0.95 | 0.61 | 0.86 | 0.17 |
Table 1: Standard reporting of select FOT parameters: Trials summary. This table illustrates all measurement replicates across trials (T1-T4) and their summary statistics (averages and standard deviations (SD)). The average values across all trials are used to represent the test session. Common parameters are listed under Variable. Resistance (Rrs) and reactance (Xrs) are provided for whole breaths at 5, 11, and 19 Hz, as well as during inspiration at 5 Hz (Rrs5(insp) and Xrs5(insp)). Additional parameters reported include reactance area (AX) at 5 Hz, resonant frequency (Fres), and tidal volume (Vt).
| Variable | Predicted | LLN | ULN | Baseline Avg | % of Predicted | Z Score |
| Rrs5 | 3.76 | – | 4.11 | 3.43 | 91% | -0.34 |
| Rrs5 (insp) | – | – | – | 3.43 | – | – |
| Rrs11 | 2.74 | – | 3.18 | 3.19 | 116% | -0.33 |
| Rrs19 | 3.52 | – | 3.92 | 3.27 | 93% | -0.3 |
| Rrs5-19 | 0.14 | – | – | 0.16 | 118% | 0.05 |
| Xrs5 | -1.37 | -1.50 | – | -0.81 | 59% | 1.32 |
| Xrs5 (insp) | – | – | – | -1.07 | – | – |
| Xrs5 (exp) | – | – | – | -0.60 | – | – |
| Delta Xrs5 | – | – | – | -0.47 | – | – |
| Xrs11 | -0.14 | -0.26 | – | -0.05 | 36% | 0.22 |
| Xrs19 | – | – | – | 0.96 | – | – |
| AX | 4.08 | 5.11 | 2.61 | 64% | -0.64 | |
| Fres | 12.73 | – | 13.14 | 11.36 | 89% | – |
Table 2: Standard reporting of select FOT parameters: Reference and predicted values. There is currently no consensus on which FOT parameters to include in a basic report; however, the ERS Technical Standard provides an example of what parameters might be reported4, which are included in the accompanying table. This table illustrates the averaged measurement values reported from the test session as well as the accompanying reference values currently available. Common parameters are listed under Variable. Resistance (Rrs) and reactance (Xrs) are provided for whole breaths at 5, 11, and 19 Hz, as well as during inspiration at 5 Hz (Rrs5(insp) and Xrs5(insp)). Additional parameters reported include reactance area (AX) at 5 Hz and resonant frequency (Fres). For those parameters with reference values available14, predicted, % predicted, lower and upper limits of normal (LLN, ULN), and Z-score values are also calculated.
| Pre-Bronchodilator | Post-Bronchodilator | |||||||||
| Variable | T1 | T2 | T3 | Avg | SD | T1 | T2 | T3 | Avg | SD |
| Rrs | 3.34 | 3.21 | 3.42 | 3.32 | 0.11 | 1.81 | 1.89 | 1.69 | 1.80 | 0.10 |
| Xrs | -1.25 | -0.72 | -0.98 | -0.98 | 0.26 | -0.42 | -1.32 | -0.74 | -0.83 | 0.45 |
| AX | 2.50 | 2.02 | 2.79 | 2.44 | 0.39 | 0.73 | 1.95 | 1.01 | 1.23 | 0.64 |
Table 3: Interpreting low-frequency resistance (Rrs), reactance (Xrs), and reactance area (AX): Trials summary. This table illustrates all measurement replicates across trials (pre- and post-bronchodilator) and their summary statistics (averages and standard deviations (SD)). The average values across all trials are used to represent the test session's values for baseline averages (pre-bronchodilator) and post-bronchodilator averages.
| Variable | Predicted | LLN | ULN | Baseline Avg | % of Predicted | Post BD Avg | % of Predicted | Absolute Change | % Change |
| Rrs | 2.14 | NA | 2.59 | 3.32 | 155% | 1.80 | 84% | 1.52 | -45.78% |
| Xrs | -0.97 | -1.11 | NA | -0.98 | 101% | -0.83 | 86% | -0.15 | 15.31% |
| AX | 2.15 | NA | 3.08 | 2.44 | 113% | 1.23 | 57% | 1.21 | -49.59% |
Table 4: Interpreting low-frequency resistance (Rrs), reactance (Xrs), and reactance area (AX): Reference and predicted values. Low-frequency (4 Hz) Rrs, Xrs, and AX are reported along with the corresponding predicted values, % of predicted, and the lower (LLN) and upper (ULN) limits of normal14. Measurements before (Baseline Avg) and after (Post BD Avg) bronchodilator are presented along with their corresponding absolute and relative change (% Change).
