A 50-year-old man with upper abdomen discomfort and chronic malnutrition had a 3.2 cm x 2.5 cm tumor in the pancreatic neck identified. He had previously been healthy and had a normal BMI (19.9 kg/m2).
No distant metastasis, major vessels (besides the splenic artery and vein), or lymph node infiltration were detected on the preoperative imaging evaluation. Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) was performed to confirm the pathological diagnosis of PDAC. The patient underwent four cycles of neoadjuvant chemotherapy using gemcitabine plus nab-paclitaxel program. The medication helped to ease clinical symptoms, and carbohydrate antigen 199 (CA-199) decreased from 4,666 U/mL to 1,350 U/mL, while the tumor's maximal diameter decreased from 3.2 cm to 2.5 cm (see Figure 3).
The outcome of the surgery is presented in Table 1. The total time for the procedure was 240 min, with a blood loss of 50 mL. The patient's recovery was uncomplicated, and he was discharged on the 9th day after the surgery. On postoperative day 3 (POD 3), the amylase level in the drainage fluid was 1,645 U/L. The drain was removed in POD 7 when the amylase level was 54 U/L. This was graded as grade A POPF. No peritoneal fluid was found on the postoperative CT examination on POD 7 (see Figure 4). The patient recovered well and was discharged on POD 9.
Histopathology revealed a moderately poorly differentiated ductal adenocarcinoma with interstitial fibrosis, thus confirming the preoperative diagnosis. The pancreatic interstitial fibrosis may be due to preoperative neoadjuvant chemotherapy (see Table 1). The resection margins of the pancreatic neck and posterior peritoneum were microscopically radical (R0). Only 15 lymph nodes were detected, and none of those were involved. The tumor was staged as T2N0M0 (AJCC 8th edition). The patient underwent six cycles of adjuvant chemotherapy using gemcitabine plus nab-paclitaxel program.
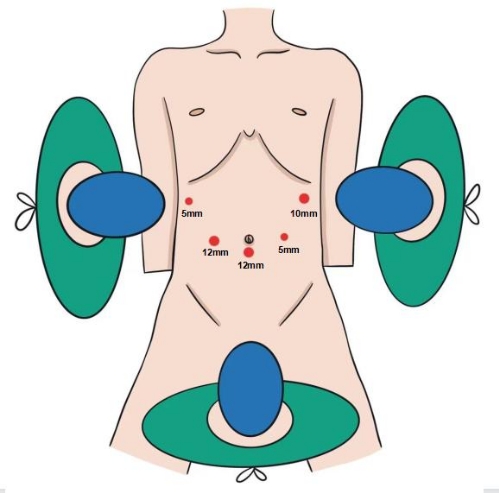
Figure 1: The position of the surgeons. The first surgeon is to the patient's right, the first assistant is to the left, and the second assistant, who is holding the laparoscope, is between the patient's legs. The procedure is performed using a five-port technique. Please click here to view a larger version of this figure.
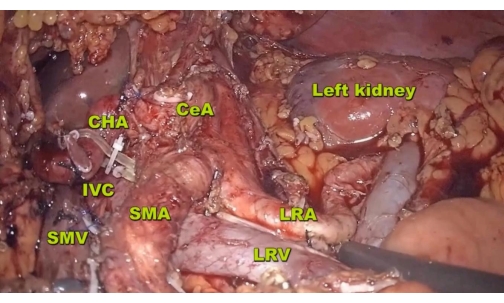
Figure 2: Resection. The resection range extends up to the diaphragmatic crus, down to the LRV, and to the posterior left lateral part of the aorta on the posterior side. Abbreviations: LRA = left renal artery, IVC = inferior vena cava. Please click here to view a larger version of this figure.
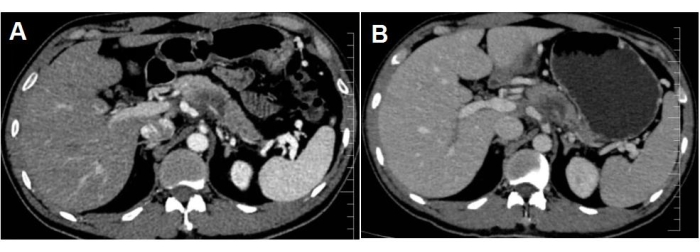
Figure 3: The images show the mass in the pancreatic neck. After neoadjuvant chemotherapy, the tumor maximum diameter was reduced from (A) 3.2 cm to (B) 2.5 cm. Please click here to view a larger version of this figure.
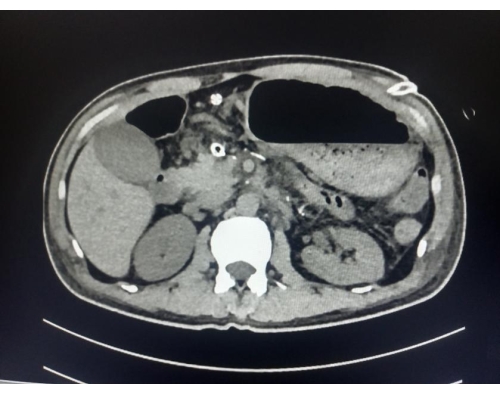
Figure 4: The CT image shows no peritoneal fluid was found on POD 7. Please click here to view a larger version of this figure.
| Variable | Outcome |
| Intraoperative | |
| operative time,minutes | 240 |
| Intraoperative blood loss,mL | 50 |
| Postoperative | |
| Postoperative pancreatic fistula(POPF) | Grade A |
| Drain removal,postoperative day | 7 |
| Postoperative hospital stay,days | 9 |
| Pathological diagnosis | Radically(R0) resected ductal adenocarcinoma with interstitial fibrosis,2cm |
Table 1: Representative outcome of the surgery.
