The success of injection was confirmed by radiologic and immunohistochemical means. Animals that underwent hemoglobin injection developed moderate acute ventriculomegaly when assessed via MRI (Figure 2A), with significantly larger lateral ventricles at 24 h and 72 h post hemoglobin injection compared to aCSF-injected animals (Figure 2B,C). While there was no significant difference in lateral ventricle volume between hemoglobin-injected and aCSF-injected animals 38 days post injection (Figure 2D), it is important to note that 44% (4/9) of the animals in the hemoglobin-injected group that were followed to 38 days post injection displayed unresolved ventriculomegaly at this timepoint (Figure 2D). This wide distribution in ventricle sizes is a pattern that is consistent with the clinical course of IVH-PHH. In addition, white matter volume was quantified at 38 days post injection (Figure 3) and was significantly decreased in the hemoglobin-injected group compared to the aCSF-injected group (Figure 3B).
We previously published a study detailing the acute inflammatory reaction that occurs after hemoglobin injection9. In this present study, proinflammatory cytokines were evaluated for tumor necrosis factor-alpha (TNFα) production in vivo (Figure 4), and immune cell infiltration into the periventricular areas and white matter were evaluated using glial fibrillary acidic protein (GFAP) immunofluorescence (Figure 5). Injection of 15 µL of hemoglobin, whole blood, or saline into the lateral ventricle of postnatal day 5 rats resulted in higher levels of proinflammatory cytokine TNFα 3 h after hemoglobin injection compared to whole blood and saline (Figure 4). There were significantly more reactive astrocytes in the corpus callosum of hemoglobin-injected animals compared to aCSF-injected animals (Figure 5). Finally, other blood breakdown products have been utilized in this fashion including iron and ferritin to reliably result in ventriculomegaly and hydrocephalus6,7.
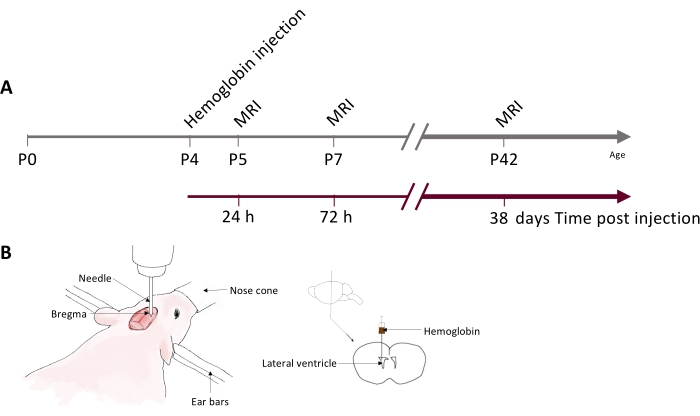
Figure 1: Experimental timeline and schematic of the neonatal rat IVH model. (A) Schematic showing hemoglobin injection and MRI timeline used for data generated in this study. (B) Schematic of stereotactic setup for injection (left) and hemoglobin injection location into the right lateral ventricle (right). Abbreviations: IVH = intraventricular hemorrhage; MRI = magnetic resonance imaging; PN = postnatal day N. Please click here to view a larger version of this figure.
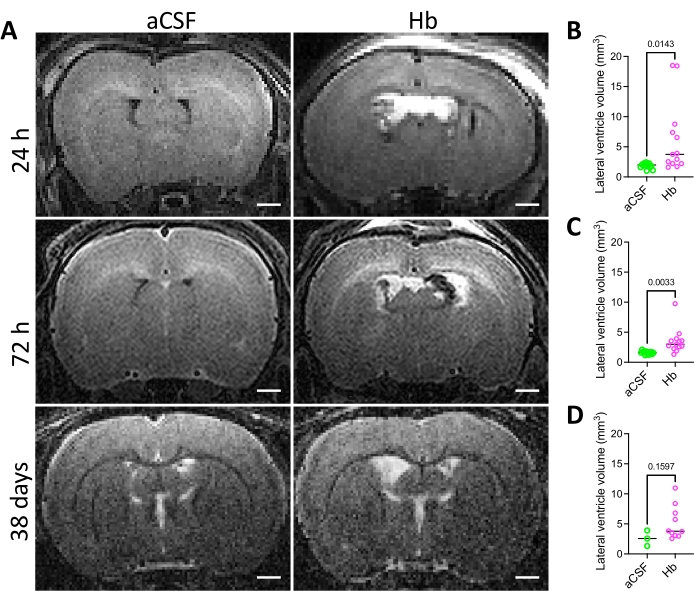
Figure 2: Lateral ventricle volumes in the intraventricular hemorrhage rat model. (A) Representative in vivo T2 coronal MRI images of rat brains 24 h, 72 h, and 38 days after intraventricular injection of aCSF (left) or 150 mg/mL Hb (right) into the right lateral ventricle at postnatal day 4. Scale bars = 1 mm. (B–D) Quantification of lateral ventricle volumes (B) 24 h, (C) 72 h, and (D) 38 days following aCSF or Hb injection. Hb-injected animals had significantly larger ventricles at 24 h and 72 h. Data in B and C are mean ± s.e.m., n = 13 per group, unpaired two-tailed t-test. Data in D are mean ± SEM, n = 3 in aCSF group and n = 9 in Hb group, unpaired two-tailed t-test. Abbreviations: MRI = magnetic resonance imaging; PN = postnatal day N; aCSF = artificial cerebrospinal fluid; Hb = hemoglobin; SEM = standard error of the mean. Please click here to view a larger version of this figure.
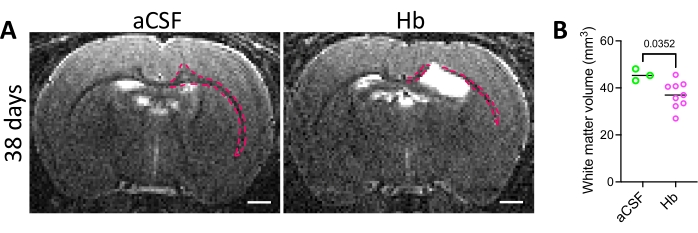
Figure 3: White matter injury in the intraventricular hemorrhage rat model. (A) Representative in vivo T2 coronal MRI images of rat brains 38 days after intraventricular injection of aCSF (left) or 150 mg/mL Hb (right) into the right lateral ventricle at postnatal day 4. White matter is outlined in red. Scale bars = 1 mm. (B) Quantification of white matter volumes 38 days following aCSF or Hb injection. Hb-injected animals had decreased white matter volumes. Data in B are mean ± SEM, n = 3 in aCSF group, n = 9 in Hb group. Unpaired two-tailed t-test. Abbreviations: MRI = magnetic resonance imaging; PN = postnatal day N; aCSF = artificial cerebrospinal fluid; Hb = hemoglobin; SEM = standard error of the mean. Please click here to view a larger version of this figure.
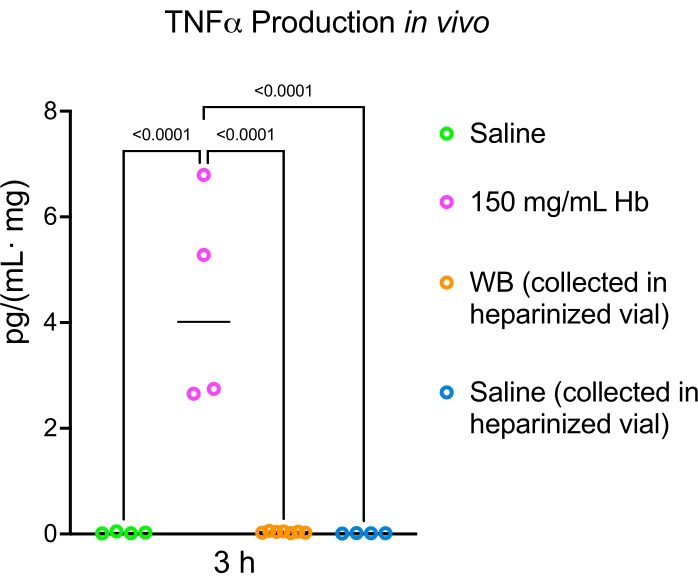
Figure 4: Hemoglobin induces more TNFα production than whole blood in vivo. Administration of 15 µL of hemoglobin, whole blood, or saline into the lateral ventricle of postnatal day 5 rats resulted in higher levels of the proinflammatory cytokine TNFα 3 h after hemoglobin injection compared to whole blood and saline. Data are mean ± SEM, n = 4 in all groups, one-way ANOVA with post-hoc Tukey's test. Abbreviations: Hb = hemoglobin; TNFα = tumor necrosis factor-alpha; WB = whole blood; ANOVA = analysis of variance. Please click here to view a larger version of this figure.
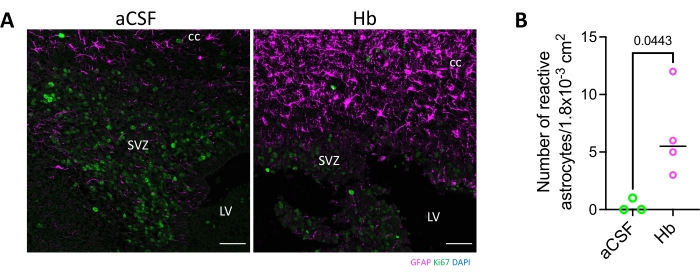
Figure 5: Astrocyte activation in the corpus callosum following hemoglobin injection into the lateral ventricle. (A) GFAP immunostaining shows hemoglobin injection into the lateral ventricle of postnatal day 4 rodents resulted in astrocyte activation in the corpus callosum and subventricular zone 72 h following injection. Scale bars = 50 µm. (B) The number of reactive astrocytes was significantly increased in hemoglobin-injected animals compared to aCSF-injected animals. Data are mean ± SEM, n = 3 in aCSF group, n = 4 in Hb group, unpaired two-tailed t-test. Abbreviations: GFAP = glial fibrillary acidic protein; DAPI = 4',6-diamidino-2-phenylindole; LV = lateral ventricle; SVZ = subventricular zone; cc = corpus callosum; aCSF = artificial cerebrospinal fluid; Hb = hemoglobin; SEM = standard error of the mean. Please click here to view a larger version of this figure.
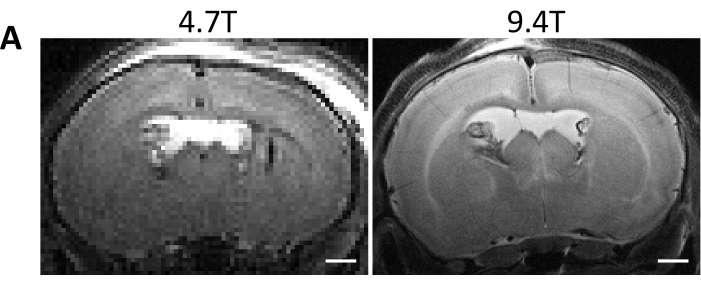
Figure 6: Comparison of 4.7T and 9.4T MRI image quality. (A) 4.7T and 9.4T T2-weighted MRI taken 72 h following hemoglobin injection into the right lateral ventricle of postnatal day 4 rats. Scale bars = 1 mm. Abbreviation: MRI = magnetic resonance imaging. Please click here to view a larger version of this figure.
