TTC staining
Heart sections from rats that underwent either the existing or improved MIRI procedure or sham surgery were stained with TTC, and the images were stored digitally and analyzed using ImageJ. Rats that underwent either the already existing or improved MIRI procedures had myocardial infarctions, while rats from the sham group did not (Figure 2B). Compared to rats in the sham group, rats in the existing (p < 0.0001) and experimental (p < 0.0001) MIRI model groups had a significant difference in myocardial infarct size, and the experimental model group had a larger myocardial infarct size than the existing model group (p = 0.0176) (Figure 3B).
Histological staining
Analysis of specimens stained using H&E and Masson stains22,23 showed that compared to the sham group, the cardiomyocytes of both the experimental and the existing model groups had experienced critical damage and nucleolysis and were infiltrated by numerous neutrophils (Figure 3).
ECG test
The ECG ST-T segments of rats in the existing and experimental MIRI model groups were elevated compared with those of rats in the sham group (Figure 4A), and the differences between the experimental model and sham groups (p < 0.0001) or the existing model and sham groups (p < 0.0001) were significant (Figure 4B). Furthermore, the ST-T segment was more elevated in the experimental model group than in the existing model group (p = 0.0274) (Figure 4C).
Percent survival
The survival rate was significantly different between the two MIRI model groups (Figure 4D). Four of the ten rats died in the existing model group. The mortality rate was 40% during the reperfusion period. In contrast, none of the rats in the experimental model group died during surgery, demonstrating that the current improved model had a higher survival rate (p = 0.0291).
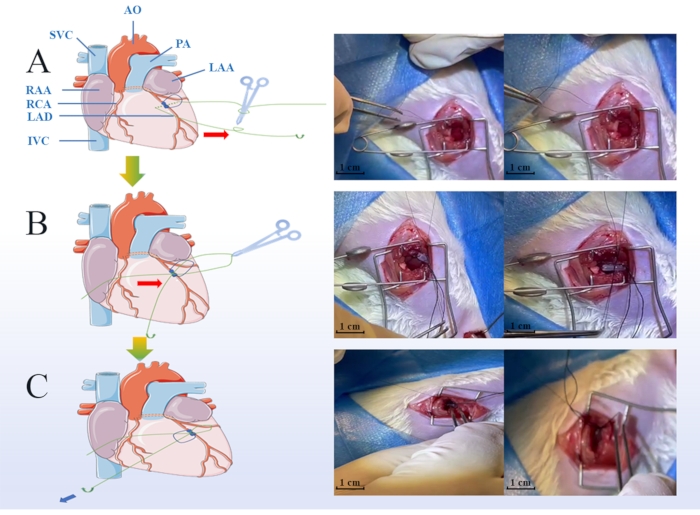
Figure 1: Key steps of the myocardial ischemic and reperfusion injury (MIRI) model surgery. Green points indicate the protocol of ligature during the ischemic period, including placing the soft tube on the coronary arteries (A), hooking the suture line into the groove of the pre-prepared soft tube (B), loosening the slipknot, and removing the soft tube when the reperfusion period was started (scale bar = 1 cm) (C). LAA: Left Atrial Appendage, RAA: Right Atrial Appendage, LAD: Left Anterior Descending, RCA: Right Coronary Artery, IVC: Inferior Vena Cava, SVC: Superior Vena Cava, AO: Aorta Artery, PA: Pulmonary Artery. Please click here to view a larger version of this figure.
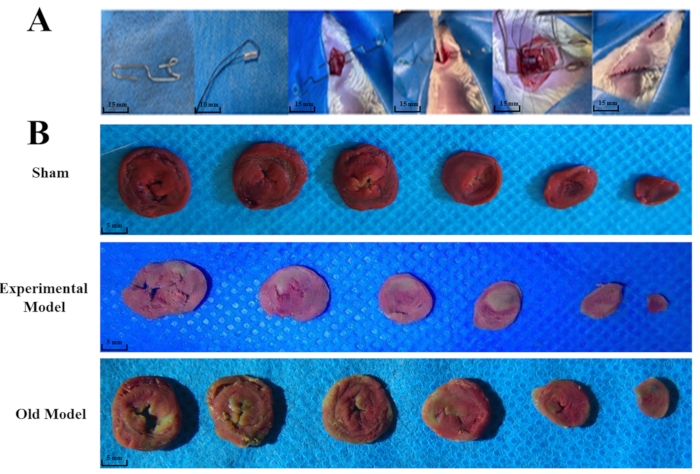
Figure 2: The whole surgery procedure and differences in triphenyltetrazolium chloride (TTC) staining between different groups. The pre-prepared small retractor (scale bar = 15 mm), soft tube (scale bar = 10 mm), and the whole surgery (scale bar = 15 mm) are shown (A). Thirty rats were randomly divided into the experimental (n = 10), sham group (n = 10), and existing model (n = 10) groups. TTC staining indicated that both the experimental and existing models' groups had significant changes compared to the sham group (B). The anterior wall of the myocardium in the experimental and the lateral wall in the existing model groups turned pale white, confirming the ischemic area's location (scale bar = 5 mm). The "existing model" is depicted as the "old model" in the figure. Please click here to view a larger version of this figure.
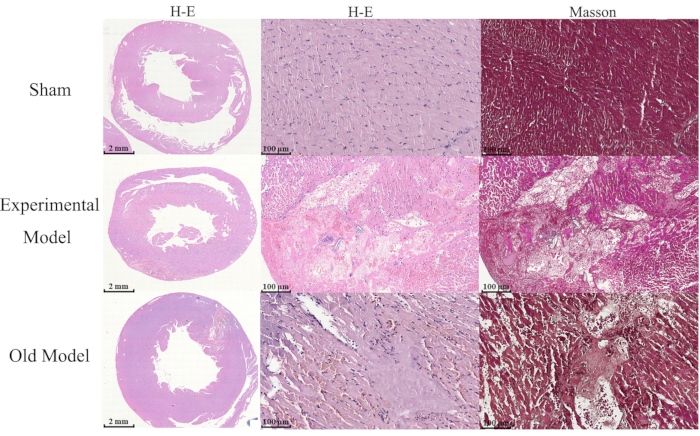
Figure 3: Differences in H&E and Masson staining between groups. Thirty male Sprague Dawley rats were randomly divided into the experimental (n = 10), sham group (n = 10), and existing model (n = 10) groups, and the comparison of cell morphological changes between groups is shown (scale bar = 2 mm). Hematoxylin and Eosin (H&E), and Masson staining show that myocardial cells of the experimental model and existing model groups have critical damage, nucleolysis, and are infiltrated by numerous neutrophils compared to those of the sham group (scale bar = 100 µm). The "existing model" is depicted as the "old model" in the figure. Please click here to view a larger version of this figure.
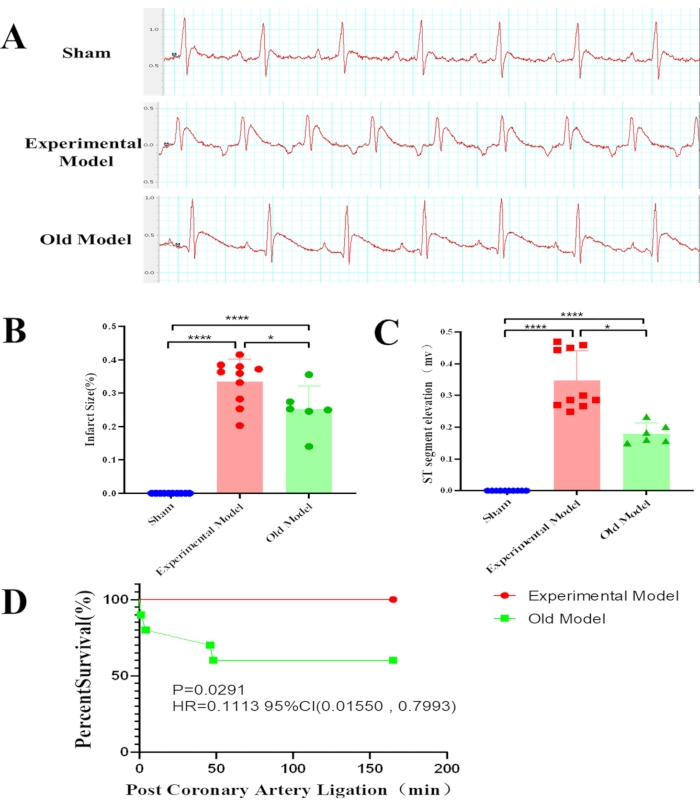
Figure 4: Differences in statistical results between groups.Thirty male Sprague Dawley rats were randomly divided into the experimental (n = 10), sham group (n = 10), and existing model (n = 10) groups. Electrocardiogram findings show that compared to the already existing model group, the experimental model group has a larger myocardial infarct size (****p < 0.0001, *p = 0.0176) (A), a higher ST-segment elevation (****p < 0.0001, *p = 0.0274) (B), and a higher survival percentage (p = 0.0291) (C). Especially, rats of the existing model group were more likely to die at the beginning of the ischemia period and the beginning of the reperfusion period (D). The "existing model" is depicted as the "old model" in the figure. Please click here to view a larger version of this figure.
Supplementary Figure 1: The details of the pre-prepared retractor and PVC tube. The pre-prepared retractor (A) and PVC tube (B) are shown. Please click here to download this File.
