Summary
The present protocol describes traumatic peripheral nerve injuries (TPNIs), including precisely calibrated crush, strictly aligned and misaligned laceration, as well as grafted and non-grafted gaps of the sciatic nerve in mice. Custom-designed sensors are developed to gauge nerve trauma, induced with commonly available tools to ensure reproducible post-TPNI outcomes.
Abstract
Traumatic peripheral nerve injury (TPNI) is a common cause of morbidity following orthopedic trauma. Reproducible and precise methods of injuring nerve and denervating muscle have long been a goal in musculoskeletal research. Many traumatically injured limbs have nerve trauma that defines the long-term patient outcome. Over several years, precise methods of producing microsurgical nerve injuries have been developed, including crush, lacerations, and nerve-gap grafting, allowing for reproducible outcome assessments. Moreover, newer methods are created for calibrated crush injuries that offer clinically relevant correlations with outcomes used to assess human patients. The principles of minimal manipulation to ensure low variability in nerve injury allow for adding still more associated tissue injuries into these models. This includes direct muscle crush and other components of limb injury. Finally, atrophy assessment and precise analysis of behavioral outcomes make these methods a complete package for studying musculoskeletal trauma that realistically incorporates all the elements of human traumatic limb injury.
Introduction
Traumatic peripheral nerve injury (TPNI) is a common cause of morbidity after orthopedic trauma1,2,3. Yearly, approximately 3% of trauma patients suffer nerve injury1,4, at an incidence of 3,50,000 cases5, resulting in 50,000 surgical repairs6. TPNIs occur in a wide range of severity, and the functional recovery directly depends on the type and severity of these injuries7,8,9. Less severe trauma (e.g., mild crush, incomplete laceration, etc.) will injure the myelin sheath and axons first, while more severe forces (e.g., severe crush, complete lacerations, etc.) will disrupt the connective nerve tissues; for example, the endoneurium, perineurium, and epineurium in addition to the myelin and axons1,10. Patients with TPNI hope that nerve function will eventually return, and muscle atrophy will be reversed. Decades of research have provided no precise treatments to enhance or ensure complete recovery despite advances in the treatment procedures11,12.
Nerve transections will not heal without surgical repair, which is often performed under the microscope. Repairs are typically performed end-to-end, making an effort to ensure that the repair site is under no tension. Nerve grafting is used to ensure that repairs are tensionless13,14. Despite the seemingly advanced methods used in these repairs, functional recovery is generally unimpressive11,12. Rehabilitation is often incomplete and unsatisfying. The optimal functional recovery requires regenerating axons to cross the injury site (nerve bridge) and innervate the target organ. These processes are complicated by axonal misdirection or growth stunting, resulting in muscle atrophy and eventual failure to recover15,16,17,18. It has been shown that functional outcomes following nerve repair (e.g., end-to-end suturing, isografting, etc.) depend on the accuracy of fascicular apposition19,20. Proper directionality of the transected nerve stumps and their fascicles is thus critical in nerve repair, without which poor functional recovery can be expected even with optimal axonal regeneration. Microsurgical suture repair itself is a traumatic process, and little has occurred in terms of novel methods to improve outcomes drastically. The field lacks reproducible nerve transection animal models, which result in predictable gaps that allow reliable recovery measurements on a functional and tissue level. Such methods, if available, would allow characterization of nerve regeneration without the problems of variable changes in neural vascularization and post denervation atrophy21,22. Many groups endeavor to use better models that limit this kind of variability. One way is to ensure that nerve repairs are minimally manipulated, and nerve stumps are perfectly opposed.
This is best accomplished by using a standardized peripheral nerve transection technique called stepwise cut and fibrin glue (STG). Repairs in this STG model are secured with fibrin glue, and gap distances are standardized and minimized21,22. Fibrin glue itself is employed in humans for these repairs, likely for the same reasons, along with its beneficial effects on post-repair scar formation23,24. The key to the present method is that the nerve repair begins before the laceration is completed, ensuring a fixed injury pattern. This current method exhibited a close commonality to the characteristic pathophysiology of nerve transection with the gold-standard epineural suturing, and the negative impact of fibrin glue was not observed on nerve regeneration. Repairing of the sciatic nerve transection with fibrin glue in mice ameliorates the elongation of axon compared to early nerve regeneration via suturing, and these findings are consistent with STG. STG also benefits from the minimal manipulation principle, where the nerve is never touched for suture positioning21. This effectively standardizes the nerve trauma associated with repair in the model. Similar principles were used to investigate misalignment by flipping the nerve before gluing22. This allowed direct comparison of nerve injuries where almost the same amount of manipulation contributed to differences in alignment without increased gap or trauma. This facilitated the direct examination of the effect of alignment on nerve-injury-induced neurovascular changes21,22, muscle atrophy21,22, and functional recovery21,22. The present investigation is all that allows the study of purposefully and precisely misaligned nerve stumps.
Most of the nerves in TPNI are not severed, have no gap or defect, and seem to be capable of recovery, and yet in many of these cases, limbs remain permanently dysfunctional from nerve injuries and confound interventions. Experimental TPNIs are customarily performed on rodent sciatic nerve crush injuries (SNCIs) using locking needle drivers (NDs), forceps, or similar devices, and an experienced surgeon to create a precise and reproducible crush injury25,26,27,28,29,30. SNCI animal models depend on innate operator precision to limit pressure variation, but this is never measured explicitly. This results in variability between animals and studies, with no clear guidance on the standardized pressure. It is thus anticipated that the capability to precisely deliver and report a coherent, accurate series of injuries with various known intensities may benefit the TPNI field. A perfect model can provide an SNCI of a known nerve injury severity to each animal by any lab or researcher for authentic inter-study and device replicability. To address this deficiency, a unique calibrated digital device was constructed containing a Force Sensitive Resistor (FSR), proficient in reporting the pressure (real-time) applied to a nerve. This device was then tested for the replicability of various crush injury pressures deployed by diverse types of forceps and NDs31.
Finally, a specific method was developed to address gaps in nerve32. The nerve gaps in the literature are induced by removing a nerve section and then repairing it back into the defect13,33,34. The manipulation required for this surgical procedure is often compounded with suturing, and the stumps of the nerve retract variably21,32,34. It was based on the reasoning that using isogenic oversized nerve grafts, the nerve stump retraction will never an issue32. The method required the simultaneous operation on two or three animals at once, taking a 7 mm graft to place into a 5 mm defect induced in another animal. The defect size of the second animal was then used to graft a still smaller defect in another animal if needed. This resulted in a comprehensive method for simultaneous surgery to graft defects with donor nerves that are always larger than the nerve defect to ensure tensionless repair. On coupling with the requirement of minimal manipulation, this offers an avenue to study graft length directly in syngeneic animals without asymmetric graft gaps that are ubiquitous in the literature20,32,34.
Protocol
The experimental design and animal protocols were approved by the Institutional Animal Care and Use Committee (IACUC) at Penn State University College of Medicine. Adult C57BL/6J male mice, 10-week-old, weighing 20-25 g, were used for the studies. Animals were housed at the animal facility under sterile animal management conditions, and they were acclimatized at least 5 days before conducting the studies.
1. Animal preparation
- Anesthetize the animals deeply using a cocktail of ketamine (100 mg/kg) and xylazine (10 mg/kg) via intraperitoneal injection using a 26 G needle.
- Shave the animals' right hind limb and lower back using a trimmer and then clean with alcohol prepped with 10% povidone-iodine solution using sterile cotton-tipped applicators (see Table of Materials).
- Apply ophthalmic lubricant ointment to the eyes using sterile cotton-tipped applicators to avoid dryness of the eyes.
- After prepping, place the animals on a homeothermic heating pad (see Table of Materials) to maintain the body temperature at 37 °C.
- Tape the mice's hind limbs on the heating pad and carefully position them symmetrically so that the knee joint makes a right angle with the body.
- Sterilize all the surgical tools by autoclaving and then place them on the sterile pad.
NOTE: The surgeon must wear a sterile mask, gown, and gloves before conducting surgeries.
2. Traumatic Peripheral Nerve Injury (TPNI) model generation
- After preparation, make a lateral skin incision (~2 cm) along the length of the femur using a scissor and a precision stereo zoom binocular microscope (see Table of Materials).
- Bluntly expose the sciatic nerve (SN) through the iliotibial band using dissecting scissors and microsurgical forceps. Avoid any iatrogenic mechanical damage to the SN.
- Close the skin with surgical staples after TPNI surgeries (steps 4-9). Administer slow-release buprenorphine (0.05 mg/kg) (see Table of Materials) subcutaneously to all the animals as an analgesic.
- Perform Sciatic Nerve Crush Injury (SNCI) following the steps below.
- Position the SN approximately 3 mm proximal to the trifurcation in the flat shape between the forceps tips (Figure 1A).
NOTE: Extreme care needs to be taken to avoid misshapen position, which brings variations in the experimental results between animals/groups. - Perform the SNCI using calibrated forceps and custom aluminum jigs (Figure 1C)31,35 to result in a specific pressure over a fixed width (3.5 mm).
NOTE: The details of the digital pressure sensor device for SNCI using calibrated forceps and custom boring jigs are mentioned in our previously published reports31,35. Custom jigs were made by boring holes in small pieces of aluminum. These jigs are confirmed to produce specific pressures using a digital pressure sensor, using parts and specifications publicly available and described previously31,35. - After positioning, push the jig gently to reach the block on the forceps, and after 30 s, slowly release the jig and confirm the injury by the altered structure of the nerve (Figure 1B).
NOTE: The structural alterations of the nerve confirm the degree of injury severity. This can be verified using microscopy in trial cases. - After SNCI, burry the nerve between the muscles carefully to avoid iatrogenic injury by a surgeon.
NOTE: The crush injuries caused by calibrated forceps were exact, reliable, and reproducible, which was established using precision pinch pressure sensor device31 (Figure 1D). The time course of real-time crush injury pressure by different jig with forceps is depicted in Figure 2A,B.
- Position the SN approximately 3 mm proximal to the trifurcation in the flat shape between the forceps tips (Figure 1A).
- Perform Transection and Glue (TG).
- Transect the SN completely ~3 mm proximal to the SN trifurcation using dissecting scissors.
- After transection, repair the nerve gap instantly by applying 10 µL of fibrin glue (see Table of Materials) around the transection site to limit further displacement of the severed nerve ends. The clotting time of fibrin glue was ~15 s.
NOTE: SN gap was uncontrolled and haphazard after transection because of retraction, which might be a variable for the resulting outcome.
- Perform Stepwise Transection and Glue (STG).
- Transect the SN incompletely (80% of its width) ~3 mm proximal to the SN trifurcation using dissecting scissors preventing gap formation.
- Next, apply 10 µL of fibrin glue around the cut site and completely transect the remaining 20% of the nerve before complete clotting (~10 s) of the glue.
NOTE: This method effectively diminished the gap formation caused by the elastic retraction of the cut nerve ends, but it was also free from additional surgical manipulation to the nerve, unlike the TG model (Figure 3A).
- Perform Flip and Transection with Glue (FTG).
- First, transect the SN to 40% of its width from each side (Figure 3B).
- Transversely flip the distal stump and apply 10 µL of fibrin glue around the transection site.
- Next, completely transect the central 20% nerve before complete clotting (~10 s) of fibrin glue.
- Confirm the complete transection under a direct microscope.
- Perform gap and grafting of nerve following the steps below.
- In a graded nerve gap and grafting model, use pairs of mice in series for cascade syngeneic nerve grafting32 in 1 set of experiments.
- In a mouse (say, mouse #1), create a 7 mm (G-7/0) nerve gap on the right SN, where the nerve was dissected ~3 mm proximal to the SN trifurcation and 7 mm distance away from this using a sterile graduated scale (Figure 3C).
NOTE: An irreparable nerve gap was created by dissecting a 7 mm sciatic nerve without grafting. This mouse is labeled G-7/0 because a 7mm graft is taken, but no repair is performed. - After dissection, immediately transfer the transected nerve to the sterile condition of the Petri dish containing phosphate-buffered saline (PBS) and bury the proximal stump of the SN (mouse #1) underneath the muscle with 10 µL of fibrin glue.
- Next, in mouse #2, create a 5 mm nerve gap on the right SN and graft the 7 mm dissected nerve section from mouse #1 using fibrin glue (10 µL, ~10 s) at both ends (G-5/7) (Figure 3C).
NOTE: While grafting, special care needs to be taken to avoid misalignments and other iatrogenic injuries of the SN by the surgeon.
- Perform Stepwise Transection and Sutures (STS).
- Severe the sciatic nerve along 80% of its width (Figure 3D), and repair the stumps using epineural stitches of 9-0 nylon.
- After completion, severe the remaining portion of the nerve and repair using a single 9-0 nylon stitch.
- Invert the nerve to expose the backside of the laceration, and use two 9-0 nylon stitches to complete the repair.
Representative Results
The custom-made digital pressure sensor device (Figure 1D) operates by detecting the change in resistance of the FSR when a force is applied. This device senses and records the most modest pressure amounts applied to it with a response time of <5 µs, a sampling rate of 20 Hz, and a pressure range of 2.5-25 lbs31. The differences in the forceps (Figure 1C) induced SNCI (Figure 1A,B) pressure that is sensed and indicated by the pressure sensor device (Figure 1D) are represented in Figure 2A,B. The gapless microsurgical nerve repair methods of STG, FTG, Gap and grafting, and STS are illustrated in Figure 3A–D respectively21,22,32.
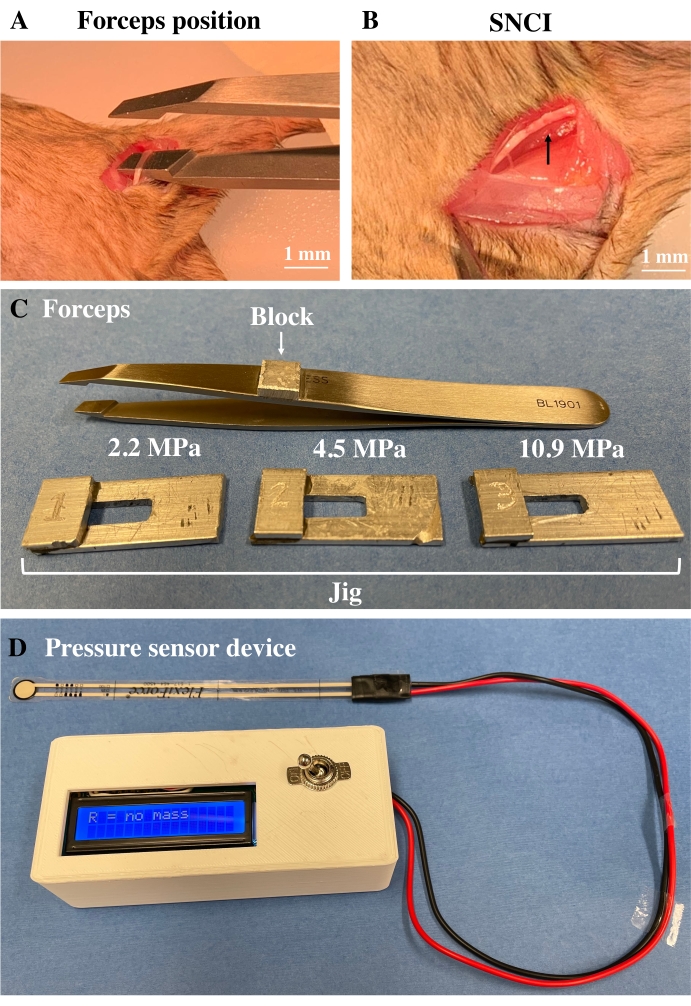
Figure 1: SNCI using calibrated forceps in the mouse. A representative image of the SN before crushing between the tip of the forceps in the flat position (A) and after crushing of SN showing the altered structure (B). (C) The calibrated forceps with a jig of different pressure (2.2, 4.5, and 10.9 MPa) were applied to the nerve. (D) Representation of the precision pinch pressure sensor device with a portable housing unit. Please click here to view a larger version of this figure.
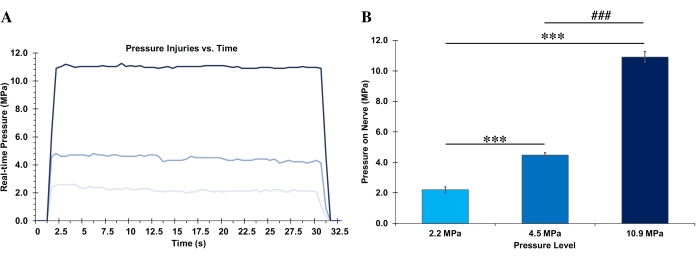
Figure 2: Real-time SNCI pressures. The tracings of time-course for real-time crush injury pressure (A) and average pressure (B) applied by forceps with different jigs during crush injury. The data were analyzed using an unpaired t-test, and all the values are presented as means ± SEM. Probability (P) values of <0.05 were considered statistically significant (***P < 0.05 for 4.5 MPa and 10.9 MPa, ###P < 0.05 for 10.9 MPa; n = 5/group). Please click here to view a larger version of this figure.
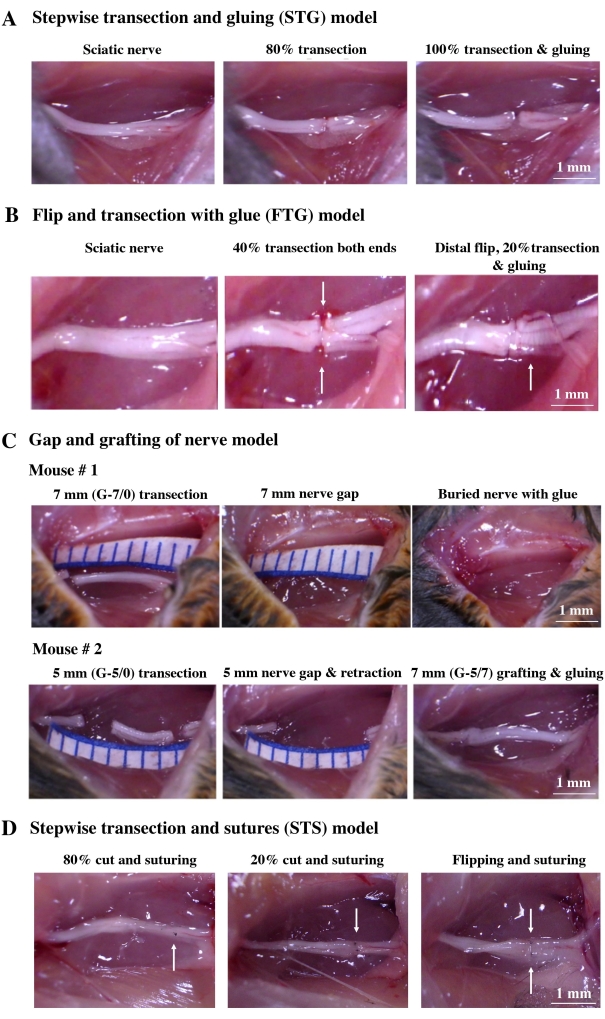
Figure 3: Gapless microsurgical nerve repair in mice. (A–D) The approach of surgical TPNI for STG, FTG, cascade syngeneic nerve grafting, and STS. (A) In STG, SN was first transected to 80% of its width to prevent gap formation between the cut ends, then 10 µL of fibrin glue is used on this partially severed portion. Then the unsevered portion of the nerve is completely severed during the hardening of the applied fibrin glue. (B). In FTG, the 80% partial laceration is achieved by cutting 40% of the nerve from either side, leaving a 20% portion unsevered in the center of the nerve (see arrow). The distal end of the nerve is then flipped over (see arrow) before applying the 10 µL of fibrin glue and severing the last 20% of the nerve while the glue hardens. (C) In G-7/0, a large gap was created by dissecting 7 mm of SN from one mouse (#1). In G-5/7, a medium-sized gap was created by dissecting the 5 mm nerve section, and the 7 mm dissected nerve section from mouse #1 (G-7/0) was then grafted and repaired with fibrin glue. (D) In STS, to prevent gap formation, SN was cut incompletely (80% of its width), then the lacerated nerve ends were repaired by epineural suture using one stitch of 9-0 nylon (see arrow). Then, the remaining portion of the nerve (20%) was transected entirely and repaired using one stitch of 9-0 nylon (see arrow). The posterior surface of the nerve was repaired using two stitches of 9-0 nylon (see arrow) after flipping over the nerve. Please click here to view a larger version of this figure.
Discussion
The history of TPNI research stretches over several decades11,12. Early experiments with dogs and larger species established the importance of animal models in the study of TPNI outcomes36,37,38. Over time, these models have moved into smaller rodents, with their established and commonly used validated outcomes measures39,40,41. Still, these models offer little standardization in terms of results, with many authors publishing varied effects with the same injuries21,26,28,29,30. This is particularly true with the sciatic nerve in mice.
There are several reasons for this variability. Nerve lacerations rarely can be repaired without a gap in the absence of extensive manipulation to place sutures21,42,43,44. The manipulation can induce additional trauma and is rarely standardized in studies. Gaps are often grafted with the excised piece of nerve from the same animal, in effect having a single animal serving as donor and recipient. This ensures that retraction will contribute to variability in gap formation. Finally, crush injury is seldom standardized.
There are techniques and tools now available to ensure injury standardization, resulting in significantly reduced variability in outcomes31. This starts with nerve crush injury, where a simple, inexpensive sensor was designed to measure the energy delivered to the nerve with fully standardized recovery measurements31. The development details and instructions for constructing these sensor devices are easy to follow and involve using simple and commercially available components31,35. This includes the simple boring of custom jigs that standardize the pressure applied to the nerve. All that is involved is ensuring enough space around the nerve so that the sensor can be positioned under the nerve before the injury. This step allows the forceps and jigs to be used in a way that guarantees a specific, recorded amount of nerve pressure.
Subsequent work proved that the outcomes got scaled with this injury severity measurement. Next, ways were found of severing nerves while ensuring that the repair was started before the nerve was severed entirely, thus ensuring strict alignment and minimal gapping at the injury site21,22. Finally, there is a unique method of gap grafting that involves simultaneous serial surgery on two or three mice at a time to ensure that gaps are always grafted with segments of a nerve that are sufficiently long32.
These techniques are easy to use and result in a much more stable outcome profile when compared to previous experience. Furthermore, the reduction in variability from these techniques allowed us to add injuries to other structures, like a muscle that had a higher fidelity to injury patterns we see in patients. One example of this was the addition of muscle injury to nerve injury, where the less variable outcomes after nerve crush allowed a muscle crush to be added to the same mode45.
While the advantages above have rendered some of the methods of studying TPNI more reliable, these methods are not without disadvantages. All of the surgical techniques presented require practice and meticulous attention to detail. The methods of SNCI carry added time for placement of the sensor in series with the nerve injury. The processes for transection that ensure reliable gap formation involves a carefully timed application of fibrin glue with completion of the injury within seconds of application. The gap grafting requires the simultaneous surgical manipulation of multiple mice at the same time. These disadvantages are notwithstanding, the key benefit is a reliable course with all the injury models presented. In many ways, the disadvantages of each injury model center on the intricacy and care required to perform it correctly. In this way, the models share the same type of disadvantage.
It is sincerely hoped that these models serve as a starting point for further developing modern injury methods that promote the critical principles of minimal manipulation and blinded assessment. This is expected to advance efforts to find treatments for severe mangling limb injuries.
Disclosures
The authors have nothing to disclose.
Acknowledgements
This work was supported by grants from the NIH (K08 AR060164-01A) and DOD (W81XWH-16-1-0725; W81XWH-19-1-0773) in addition to institutional support from the Pennsylvania State University College of Medicine, Hershey, PA 17033, USA.
Materials
| Alcohol prep | COVIDIEN | 5110 | |
| Buprenorphine | ZooPharm | BSRLAB0.5-211706 | |
| C57BL/6J | Jackson Laboratories, Bar Harbor | N/A | |
| Cotton tipped applicators | Puritan | 25-8062WC | |
| Dissecting scissor | ASSI | ASSI.SDC18R8 | |
| Fibrin glue-TISSEEL | Baxter | 1501263 | |
| Force Sensitive Resistor (FSR) | N/A | FlexiForce A301 | |
| Forceps | FST-Dumont | 5SF Inox, 11252-00 | |
| GraphPad Prism | GraphPad Software Inc. | Version 8.4.3. | |
| Homeothermic heating pad | Kent Scientific | RJ1675 | |
| Ketamine/Ketaved | VEDCO | VED1220 | |
| Microsurgical Forceps | Miltex Premium instruments | BL1901 | |
| Ophthalmic lubricant ointment | Akorn Animal Health | NDC 59399-162-35 | |
| Petri dish | VWR | 25384-092 | |
| Phosphate-buffered saline | Gibco | 14190-144 | |
| Povidone iodine | Solimo | L0017765SA | |
| Precision pinch pressure sensor device | Custom made | N/A | |
| Scissor | Miltex Premium | 21-536 | |
| Stereo zoom binocular microscope | World Precision Instruments | Model PZMIII | |
| Sterile gloves | Cardinal Health | 9L19E511 | |
| Surgical staples | 3M-Precise | DS-25 | |
| Surgical Tape | 3M-Microphore | 1530-0 | |
| Sutures | Ethicon | BV130-5 | |
| Syringe | BD syringe | 309597 | |
| Trimmer | Philips Electronics | MG3750 | |
| Xylazine/Anased | Akorn Animal Health, Inc. | VAM4811 |
References
- Robinson, L. R. Traumatic injury to peripheral nerves. Muscle & Nerve. 23 (6), 863-873 (2000).
- Campbell, W. W. Evaluation and management of peripheral nerve injury. Clinical Neurophysiology. Official Journal of the International Federation of Clinical Neurophysiology. 119 (9), 1951-1965 (2008).
- Dirschl, D. R., Dahners, L. E. The mangled extremity: when should it be amputated. The Journal of the American Academy of Orthopaedic Surgeons. 4 (4), 182-190 (1996).
- Noble, J., Munro, C. A., Prasad, V. S., Midha, R. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. The Journal of Trauma. 45 (1), 116-122 (1998).
- Barton, N., Kelsey, J., Paemer, A., Nelson, L., Felberg, A., Rice, D. Upper extremity disorders: frequency, impact and cost. Journal of Hand Surgery. 23 (2), 255 (1998).
- Evans, G. R. Peripheral nerve injury: a review and approach to tissue engineered constructs. The Anatomical Record. 263 (4), 396-404 (2001).
- Lundborg, G. . Nerve injury and repair: regeneration, reconstruction, and cortical remodeling. , (2004).
- Thieme, . Surgery of peripheral nerves: a case-based approach. , (2008).
- Brushart, T. M. . Nerve repair. , (2011).
- Menorca, R. M. G., Fussell, T. S., Elfar, J. C. Nerve physiology: mechanisms of injury and recovery. Hand Clinics. 29 (3), 317-330 (2013).
- Faroni, A., Mobasseri, S. A., Kingham, P. J., Reid, A. J. Peripheral nerve regeneration: experimental strategies and future perspectives. Advanced Drug Delivery Reviews. 82-83, 160-167 (2015).
- Zochodne, D. W. The challenges and beauty of peripheral nerve regrowth. Journal of the peripheral nervous system: JPNS. 17 (1), 1-18 (2012).
- Isaacs, J. Major peripheral nerve injuries. Hand Clinics. 29 (3), 371-382 (2013).
- Siemionow, M., Brzezicki, G. Chapter 8: Current techniques and concepts in peripheral nerve repair. International Review of Neurobiology. 87, 141-172 (2009).
- de Ruiter, G. C. W., et al. Misdirection of regenerating motor axons after nerve injury and repair in the rat sciatic nerve model. Experimental Neurology. 211 (2), 339-350 (2008).
- Gordon, T. Nerve regeneration: understanding biology and its influence on return of function after nerve transfers. Hand Clinics. 32 (2), 103-117 (2016).
- Sobotka, S., Mu, L. Muscle reinnervation with nerve-muscle-endplate band grafting technique: correlation between force recovery and axonal regeneration. The Journal of Surgical Research. 195 (1), 144-151 (2015).
- Witzel, C., Rohde, C., Brushart, T. M. Pathway sampling by regenerating peripheral axons. The Journal of Comparative Neurology. 485 (3), 183-190 (2005).
- Orgel, M. G., Terzis, J. K. Epineurial vs. perineurial repair. Plastic and Reconstructive Surgery. 60 (1), 80-91 (1977).
- Bassilios Habre, S., Bond, G., Jing, X. L., Kostopoulos, E., Wallace, R. D., Konofaos, P. The surgical management of nerve gaps: present and future. Annals of Plastic Surgery. 80 (3), 252-261 (2018).
- Lee, J. I., et al. A novel nerve transection and repair method in mice: histomorphometric analysis of nerves, blood vessels, and muscles with functional recovery. Scientific Reports. 10 (1), 21637 (2020).
- Lee, J. I., et al. Purposeful misalignment of severed nerve stumps in a standardized transection model reveals persistent functional deficit with aberrant neurofilament distribution. Military Medicine. 186, 696-703 (2021).
- Sameem, M., Wood, T. J., Bain, J. R. A systematic review on the use of fibrin glue for peripheral nerve repair. Plastic and Reconstructive Surgery. 127 (6), 2381-2390 (2011).
- Spotnitz, W. D. Fibrin sealant: the only approved hemostat, sealant, and adhesive-a laboratory and clinical perspective. ISRN surgery. 2014, 203943 (2014).
- de V. Alant, J. D., Kemp, S. W. P., Khu, K. J. O. L., Kumar, R., Webb, A. A., Midha, R. Traumatic neuroma in continuity injury model in rodents. Journal of Neurotrauma. 29 (8), 1691-1703 (2012).
- Geary, M. B., et al. Erythropoietin accelerates functional recovery after moderate sciatic nerve crush injury. Muscle & Nerve. 56 (1), 143-151 (2017).
- Răducan, A., et al. Morphological and functional aspects of sciatic nerve regeneration after crush injury. Romanian Journal of Morphology and Embryology. 54, 735-739 (2013).
- Elfar, J. C., Jacobson, J. A., Puzas, J. E., Rosier, R. N., Zuscik, M. J. Erythropoietin accelerates functional recovery after peripheral nerve injury. The Journal of Bone and Joint Surgery. American Volume. 90 (8), 1644-1653 (2008).
- Sundem, L., Chris Tseng, K. C., Li, H., Ketz, J., Noble, M., Elfar, J. Erythropoietin enhanced recovery after traumatic nerve injury: myelination and localized effects. The Journal of Hand Surgery. 41 (10), 999-1010 (2016).
- Govindappa, P. K., Talukder, M. A. H., Gurjar, A. A., Hegarty, J. P., Elfar, J. C. An effective erythropoietin dose regimen protects against severe nerve injury-induced pathophysiological changes with improved neural gene expression and enhances functional recovery. International Immunopharmacology. 82, 106330 (2020).
- Wandling, G. D., Lee, J. I., Talukder, M. A. H., Govindappa, P. K., Elfar, J. C. Novel real-time digital pressure sensor reveals wide variations in current nerve crush injury models. Military Medicine. 186, 473-478 (2021).
- Lee, J. I., Talukder, M. A. H., Karuman, K., Gurjar, A. A., Govindappa, P. K., Guddadarangaiah, J. M., Manto, K. M., Wandling, G. D., Hegarty, J. P., Waning, D. L., Elfar, J. C. Functional recovery and muscle atrophy in pre-clinical models of peripheral nerve transection and gap-grafting in mice. Effects of 4-aminopyridine. Neural Regeneration Research. , (2021).
- Lee, D. H., You, J., Jung, J. W., Park, J. W., Lee, J. I. Comparison between normal and reverse orientation of graft in functional and histomorphological outcomes after autologous nerve grafting: An experimental study in the mouse model. Microsurgery. 41 (7), 645-654 (2021).
- Lubiatowski, P., Unsal, F. M., Nair, D., Ozer, K., Siemionow, M. The epineural sleeve technique for nerve graft reconstruction enhances nerve recovery. Microsurgery. 28 (3), 160-167 (2008).
- Lee, J. I., Wandling, G. D., Talukder, M. A. H., Govindappa, P. K., Elfar, J. C. A novel standardized peripheral nerve transection method and a novel digital pressure sensor device construction for peripheral nerve crush injury. Bio-protocol. , (2022).
- Farinas, A. F., Stephanides, M., Kassis, S., Keller, P., Colazo, J. M., Thayer, W. P. Sciatic nerve injury model in rabbits: What to expect. Laboratory Animals. 54 (6), 559-567 (2020).
- Yao, Y., et al. Efect of longitudinally oriented collagen conduit combined with nerve growth factor on nerve regeneration after dog sciatic nerve injury. Journal of Biomedical Materials Research. Part B, Applied Biomaterials. 106 (6), 2131-2139 (2018).
- Schmitz, H. C., Beer, G. M. The toe-spreading reflex of the rabbit revisited–functional evaluation of complete peroneal nerve lesions. Laboratory Animals. 35 (4), 340-345 (2001).
- Bauder, A. R., Ferguson, T. A. Reproducible mouse sciatic nerve crush and subsequent assessment of regeneration by whole mount muscle analysis. Journal of Visualized Experiments. 60, 3606 (2012).
- Colleoni, M., Sacerdote, P. Murine models of human neuropathic pain. Biochimica et Biophysica Acta. 1802 (10), 924-933 (2010).
- Challa, S. R. Surgical animal models of neuropathic pain: Pros and Cons. The International Journal of Neuroscience. 125 (3), 170-174 (2015).
- M, F. G., M, M., S, H., Khan, W. S. Peripheral nerve injury: principles for repair and regeneration. The Open Orthopaedics Journal. 8, 199-203 (2014).
- Grinsell, D., Keating, C. P. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. BioMed Research International. 2014, 698256 (2014).
- Carvalho, C. R., Reis, R. L., Oliveira, J. M. Fundamentals and current strategies for peripheral nerve repair and regeneration. Advances in Experimental Medicine and Biology. 1249, 173-201 (2020).
- Govindappa, P. K., Jagadeeshaprasad, M. G., Tortora, P., Talukder, M. A. H., Elfar, J. C. Effects of 4-aminopyridine on combined nerve and muscle injury and bone loss. The Journal of Hand Surgery. , (2022).

.