Animals exposed to an adenine diet have reduced glomerular filtration rates (control: 441.3 ± 54.2 µL/min vs. CKD: 165.1 ± 118.3 µL/min, p < 0.05) and increased serum blood urea nitrogen levels (control: 20.39 ± 4.2 µL/min vs. CKD: 38.20 ± 10.65 µL/min, p < 0.05) compared to the animals that received casein-based chow, confirming the presence of kidney insufficiency prior to arteriovenous fistula surgery.
Validation of AVF patency
Although intra-operative visual confirmation of technical success is the initial identification of fistula patency, it does not fully guarantee patency or physiological maturation throughout the study period. Postoperative patency outcomes (i.e., success or failure) were determined using both duplex ultrasound imaging and histological examination, as we have previously demonstrated25. Figure 2 shows the representative B mode, pulse wave Doppler, and color Doppler ultrasound images and morphological sections of an arteriovenous fistula anastomosis, respectively. A patent fistula is directly visualized on color Doppler analysis with turbulent hemodynamics, as well as spectral broadening at the site of the fistula. Adaptive flow-mediated changes of the inflow and outflow vessels also indirectly confirm AVF patency. Specifically, the aorta has elevated peak systolic and end-diastolic velocity, the IVC develops pulsatility with elevated peak velocity, and vessel dilation in both the aorta and IVC is apparent (Figure 2A). In contrast, a failed or thrombosed fistula has almost no changes in inflow or outflow measurements and no turbulence or spectral broadening within the left iliac vasculature. Usually, fistula failure from thrombosis partially or fully occludes the left iliac artery, which is visualized as minimal to no flow on pulse-wave Doppler analysis. Figure 2B shows serial histology sections of an AVF 2 weeks after surgical creation. The sections are 5 µm thick and stained with Masson's trichrome. Surgical anastomosis of the artery and vein is obvious, and distinct venous arterialization is present (venous wall thickening and fibrosis with neointimal hyperplasia). Ultrasound imaging was performed on postoperative day 3 to rule out mice with early AVF failure, and then serial, non-invasive measurements were obtained throughout the study period. Morphological assessment provides period-specific vascular remodeling details at the time of sacrifice and was used to confirm ultrasound findings. An AVF patency rate of approximately 50% (20%-30% of postoperative death and 20%-30% of fistula failure)25 is to be expected initially, but the surgical success rate improves significantly (~5%-10% failure rate) with practice and increased proficiency.
Pathophysiological characteristics following iliac arteriovenous fistula formation
Hemodynamic alteration: Characteristics of AVF hemodynamics and distal hindlimb perfusion must be quantified to contextualize access-related limb pathophysiology. B-mode and pulse-wave Doppler ultrasound measurements after surgery revealed inflow and outflow vessel dilation (IVC: 1.4-fold at POD3 and 1.6-fold at POD13 and IRA: 1.4-fold at POD3 and 1.7-fold at POD13, p < 0.05) and increases in peak systolic velocity (IVC peak systolic velocity: 5.5-fold at POD3 and 4.9-fold at POD13 and IRA peak systolic velocity: 2.8-fold at POD3 and 3.7-fold at POD13, P < 0.05) compared to the sham animals (Figure 3A–D). Further, unilateral hindlimb ischemia was apparent postoperatively, which confirms steal-mediated arterial hypoperfusion distal to the fistula. Left paw perfusion deficits are expected to be ~20% of the contralateral limb, and the perfusion deficit of the tibialis anterior muscle is ~60%. Mice partially recovered these deficits throughout the study period (Figure 3E,F).
Hindlimb dysfunction: Ipsilateral limb disability is expected after AVF creation, which involves mild (most cases) to severe (few cases) leg limping that can last for several days. Unresolved hindlimb paralysis and/or paw necrosis might be indicative of a severe ischemic insult caused by fistula size out of the normal range. Hindlimb neuromotor function was quantified via grip strength testing and treadmill gait pattern analysis, which were performed sequentially throughout the recovery period. Expected unilateral grip strength is ~50% of the contralateral limb on postoperative day 4, with gradual recovery. AVF mice also require reduced treadmill speeds during gait assessment (<20 cm/min) (Figure 3G,H).
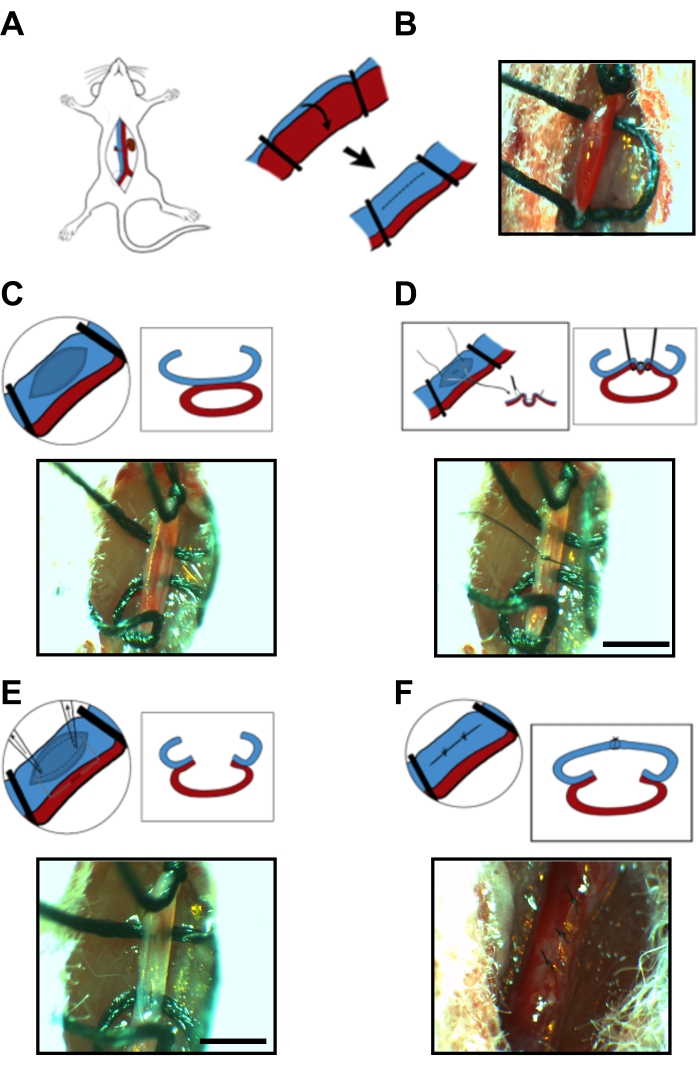
Figure 1: Microsurgery steps of arteriovenous fistula anastomosis. (A) Exposure of the surgical target area, including midline laparotomy and left iliac artery/vein isolation. (B) 4-0 suture ligatures (e.g., used as temporary vessel clamps) on the left common iliac arteriovenous bundle at proximal and distal sites. (C) A longitudinal venotomy on the anterior wall of the iliac vein. (D) 10-0 imbricating suture via the posterior wall of the iliac vein and the anterior wall of the iliac artery. (E) Elliptical incision with the imbricating distension. (F) Initial longitudinal venotomy from Image C is repaired using an interrupted 10-0 suture. Scale bar = 1 mm. Please click here to view a larger version of this figure.
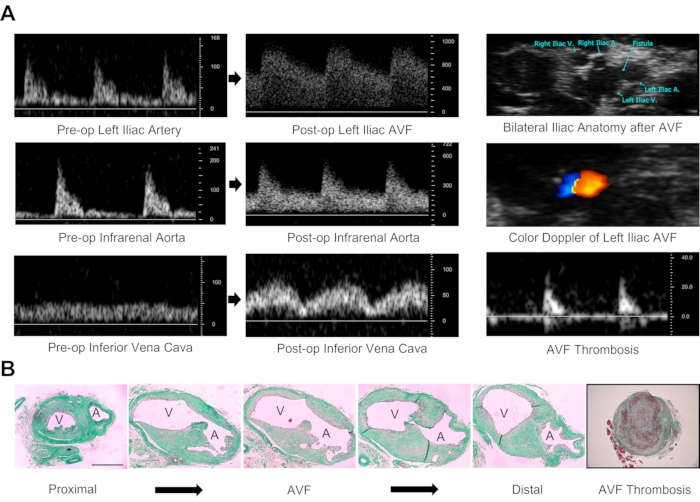
Figure 2: Validation of arteriovenous fistula patency. (A) Doppler ultrasound determination of AVF patency. Characteristics of a patent fistula include arterial and venous dilation on B-mode imaging, turbulent flow on color Doppler analysis of the left iliac vasculature, pulsatile spectral broadening on pulse-wave Doppler assessment of the left iliac vessels, increases in peak systolic and end-diastolic velocity of the infrarenal aorta, and pulsatility within the IVC with increases in peak systolic velocity. Diminished or absent flow within the iliac vessels is suggestive of AVF failure/thrombosis. The duplex ultrasound technique provides both morphological and physiological data. Velocity measurements are in millimeters per second. (B) Morphological assessment of AVF anastomosis 14 days after fistula creation. Images were stained with Masson's trichrome. There are anatomical changes in serial section microscopy from proximal (left end) to distal (right end) common iliac arteriovenous anatomy. Occlusion of the vasculature due to clot and/or excessive neointimal hyperplasia confirms AVF failure. Images are 10x magnification. A: Common iliac artery, V: Common iliac vein. Scale bar = 500 µm. Please click here to view a larger version of this figure.
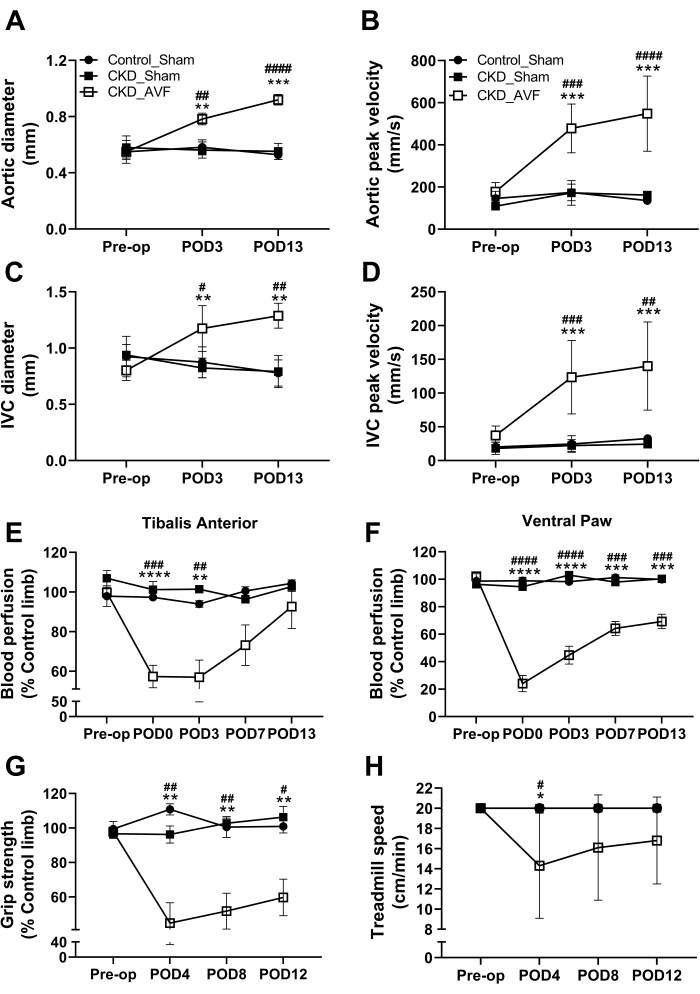
Figure 3: Pathophysiological characteristics prior to and following AVF formation. Quantification of ultrasound imaging in (A) infrarenal aortic diameter, (B) infrarenal aortic peak systolic velocity, (C) inferior vena cava diameter, and (D) inferior vena cava peak systolic velocity pre-operatively and at postoperative days 3 and 13. Local blood perfusion (Laser doppler) measurement on (E) tibialis anterior and (F) ventral paw before surgery and throughout the 2 week recovery period. Neuromotor functional testing included (G) grip strength and (H) treadmill test pre- and post-operatively. Data were analyzed using a two-way ANOVA, and Tukey's post-hoc test was performed when appropriate. Values are means ± SD. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001 vs. Control_Sham. #p < 0.05, ##p < 0.01, ###p < 0.001, ####p < 0.0001 vs. CKD_Sham. N = 6-10/group. Please click here to view a larger version of this figure.
