Large joints affected by OA are often swollen and produce significant amounts of SF, which are drained via arthrocentesis15. The macroscopic characteristics of SF evaluated immediately after arthrocentesis essentially include the quantity, color, clarity, and viscosity17. Despite their low specificity, they provide preliminary data on the degree of inflammation. The color depends on SF cellularity and the degree of fragmentation of extracellular matrix macromolecules. The SF collected from patients with OA is pale yellow, a shade generally associated with non-inflammatory samples, whereas dark yellow is associated with inflammatory effusions (Figure 2). The presence of small amounts of blood in the sample, for instance, due to capillary ruptures, results in slightly orange color. Bloody effusions must be carefully considered as they might indicate a potential hemarthrosis. Clarity is a hallmark of SF collected from patients with OA. In fact, non-inflammatory SF is poor in cells, debris, hyaluronic acid, and fibrin fragments, unlike the turbid appearance of inflammatory SF (Figure 2).
Viscosity represents a good inflammatory index as it is associated with the integrity of matrix macromolecules, mainly hyaluronic acid (Figure 2). These molecules depolymerize during inflammation, resulting in a less viscous SF. Depending on the disease stage and severity, the viscosity may be preserved or slightly reduced in OA.
The number of leukocytes never exceeds 500-1,000 cells/mm3 in OA, and they are mostly monocytes (Supplementary Figure 5A) and other mononuclear cells like synoviocytes (Supplementary Figure 5B). One of the most relevant and frequent findings in OA SF concerns CPP and BCP crystals. CPP crystals are easily detected under compensated polarized light microscopy (Figure 5), whereas the identification of BCP crystals is rendered more difficult due to their submicroscopic size (Figure 6). In fact, the length of a single BCP crystal is less than 1 µm, and although these crystals form aggregates, the clumps appear as non-birefringent amorphous-looking globules. Although nonspecific, positive alizarin red staining generally reveals the presence of BCP crystals.
Contrary to pseudogout, wherein CPP crystals are numerous and associated with high leukocyte counts and inflammatory clinical features, in OA, the number of CPP crystals in SF is very low and not linked to any altered humoral response. Nevertheless, SF samples with CPP or BCP crystals display higher levels of inflammatory cytokines when compared with OA without crystals21. Regardless of WBC count, SFs with crystals are also associated with increased percentages of PMN cells5. From a clinical point of view, the relationship between calcium crystals and inflammation may help define a particular subset of patients at an increased risk of developing more severe disease.
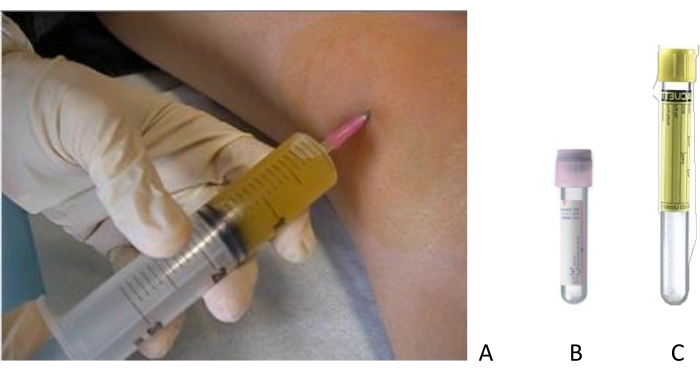
Figure 1: Joint aspiration of a swollen knee. (A) Arthrocentesis is performed after accurate disinfection of the skin with sterile materials. The SF is collected in (B) EDTA tubes for total cell count and (C) no-additive tubes for differential cell count and crystal search. Please click here to view a larger version of this figure.
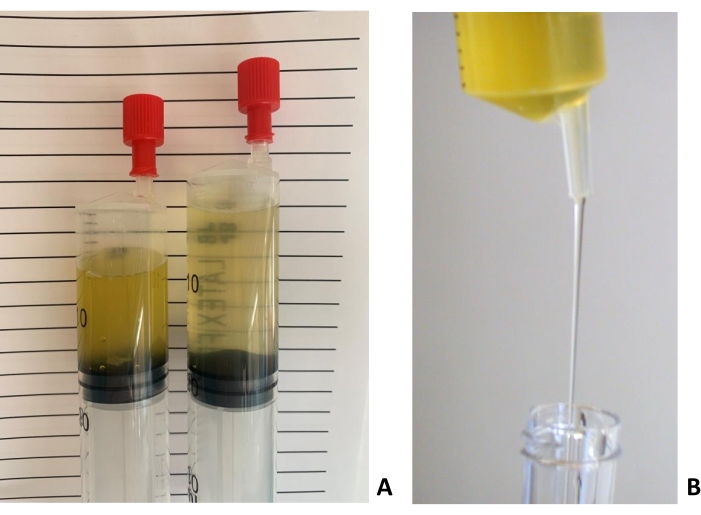
Figure 2: Characteristics of inflammatory (left) and non-inflammatory (right) SF samples. (A) Color and clarity of inflammatory (left) and non-inflammatory (right) SF samples. (B) The viscosity of a non-inflammatory SF evaluated through the "string" test. The laboratorist evaluates the length of the "string" formed by a falling drop of SF from a syringe or a pipette. The sample in the picture produces a long string. Please click here to view a larger version of this figure.
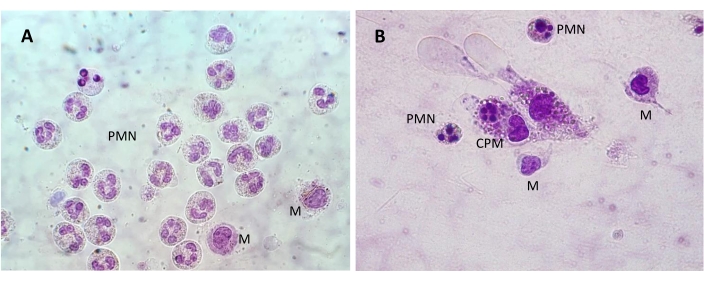
Figure 3: SF cells observed in a pre-stained slide. (A) A group of polymorphonuclear (PMN) cells with multilobed nuclei and two monocytes with their bulky nuclei in the lower right side of the image. (B) PMN cells and monocytes (M) with a cytophagocytic mononuclear (CPM) cell in the center of the image. Bright field; 1,000x magnification. Please click here to view a larger version of this figure.
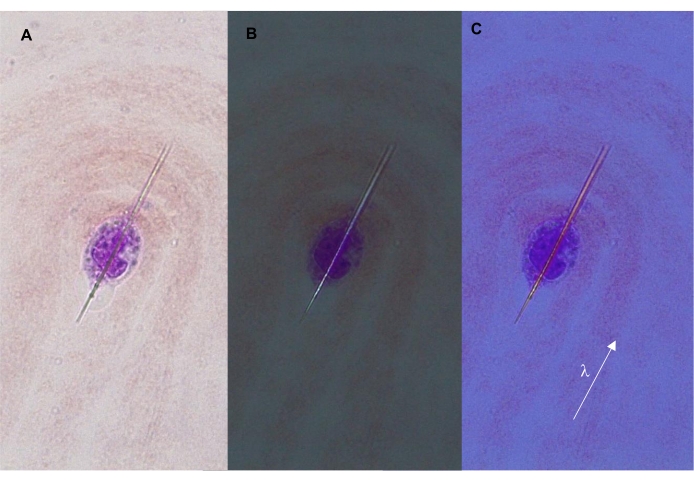
Figure 4: Intracellular MSU crystal. The crystal forms a typical needle shape shown under (A) transmitted, (B) polarized, and (C) compensated polarized light (400x). The arrow indicates the orientation of the λ filter (compensator), which is parallel to the long axis of the crystal. In this configuration, the crystal appears yellow/orange. Please click here to view a larger version of this figure.
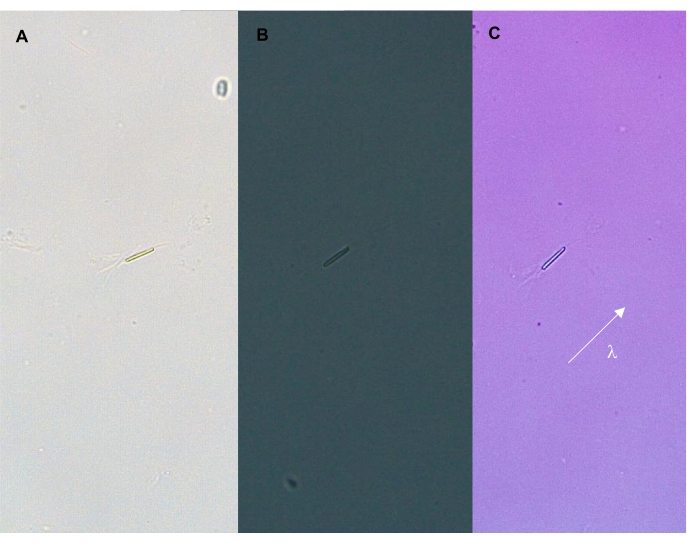
Figure 5: Intracellular CPP crystal. The crystal is shown under (A) transmitted, (B) polarized, and (C) compensated light (400x). The arrow indicates the orientation of the λ filter (compensator), which is parallel to the long axis of the crystal. In this configuration, the crystal appears blue. Please click here to view a larger version of this figure.
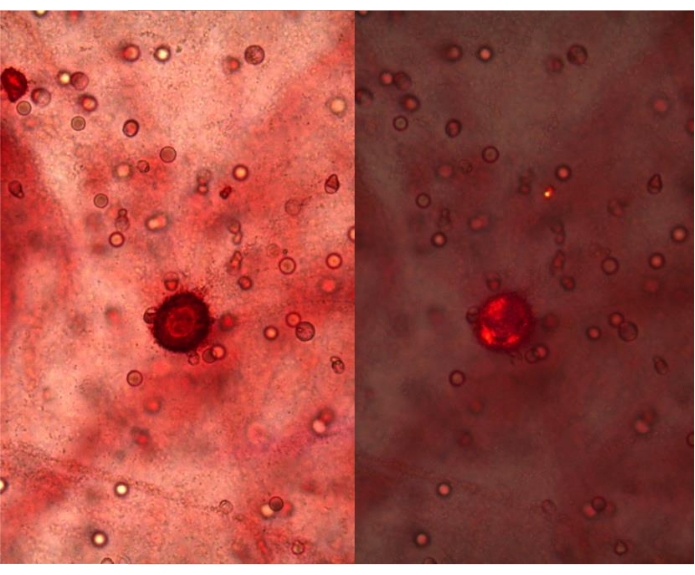
Figure 6: Positivity to the alizarin red test of an SF from OA, 400x. Red precipitates are visible under transmitted light (left panel) and polarized light (right panel), 400x magnification. Please click here to view a larger version of this figure.
Table 1: Degree of inflammation of SF according to the total number of leucocytes. Please click here to download this Table.
Table 2: Colors exhibited by MSU and CPP crystals under compensated polarized light and signs of birefringence. Please click here to download this Table.
Supplementary Figure 1: Blood diluting pipettes according to Malassez-Potain for leucocytes. Please click here to download this File.
Supplementary Figure 2: The layout of the chamber grid for WBC count. Please click here to download this File.
Supplementary Figure 3: Pre-stained, ready-to-use slides for a quick and easy differential WBC morphology evaluation. Please click here to download this File.
Supplementary Figure 4: May-Grünwald-Giemsa staining of an SF smear. Eosinophilic granules are clearly visible (arrow), 1,000x magnification. Please click here to download this File.
Supplementary Figure 5: Monocyte and synoviocytes collected from an SF sample. (A) Monocyte from an SF sample collected from a patient with osteoarthritis (1,000x). (B) Synoviocytes from an SF sample collected from a patient with osteoarthritis (1,000x). Please click here to download this File.
