With respect to interpreting the continuous venous-arterial Doppler ultrasound during a preload challenge, general physiological responses are illustrated in Figure 1, Figure 2, Figure 3, and Figure 4.
First, in a patient with a normal, upright cardiac function curve, a small increase in the cardiac preload (e.g., as inferred by jugular venous Doppler) is accompanied by a relatively large rise in the stroke volume (e.g., as indicated by ccFT augmentation)2,14,36; this is exemplified by Figure 1. Inferring changes in the jugular venous pressure (JVP) from the jugular Doppler spectrum during the preload challenge deserves some elaboration. Again, this physiological variable is a surrogate for cardiac preload or filling. Normally, the jugular vein is collapsed in the upright position when the jugular venous pressure is less than the atmospheric pressure. In the Doppler spectrum, this translates to a relatively high velocity (i.e., usually more than 50 cm/s) with minimal pulsations and low amplitude (i.e., the intensity or "brightness" of the jugular signal). Then, if the jugular venous pressure rises during the maneuver, the vein rounds out in diameter, its velocity falls (i.e., usually to less than 50 cm/s), the intensity (i.e., "brightness") increases, and the waveform becomes more pulsatile2,14,36. As shown in Figure 1, the change in the venous Doppler morphology indicates that the jugular vein has increased in diameter (i.e., falling velocity, rising amplitude) and is beginning to follow the right atrial pressure deflections. Though not pictured, with increased right atrial pressure, the "v" wave during late systole can cleave the monophasic wave seen in Figure 1 into a systolic "s" velocity wave and a diastolic "d" velocity wave2,14,36. In as-of-yet unpublished data in healthy volunteers, we observed that jugular venous Doppler morphology was the most accurate venous ultrasonographic measure for distinguishing low from high preload states.
In contrast, an abnormal response is depicted in Figure 2. A clinical example of this pathophysiology is a hypovolemic, veno-dilated, septic patient with evolving septic cardiac dysfunction2,15,36. Such a patient has diminished venous return (which reduces the cardiac preload, i.e., the right atrial or jugular venous pressure) and simultaneously depressed cardiac function2,15,35,36. Therefore, at baseline, this patient demonstrates a continuous, low-JVP venous Doppler morphology that increases (i.e., becomes more pulsatile) during the preload challenge without a significant rise in the ccFT. This effectively describes a flattened slope of the cardiac function curve.
The results from continuous venous-arterial Doppler could also alert the treating clinician to problems with the PLR itself. For example, in some situations, the PLR may not recruit enough venous blood from the lower extremities and splanchnic circulation to generate a physiologically effective preload challenge4. Without assessing the cardiac filling, this could result in a "false negative" PLR. However, if the clinician sees little ccFT response (i.e., as a stroke volume surrogate) coupled with no change in the venous Doppler (i.e., as a surrogate for preload), this could herald an ineffective PLR, as seen in Figure 3.
Lastly, it is critical that the PLR maneuver is true to its namesake, meaning that there is no exertion by the patient when the torso falls and the legs elevate13. This avoids adrenergic discharge, which may increase the cardiac function independently of the venous return; however, as described in Figure 4, this undesired scenario may be indicated by the parameters of a rising stroke volume in the arterial signal coupled with a venous Doppler morphology, suggesting diminished venous pressure.
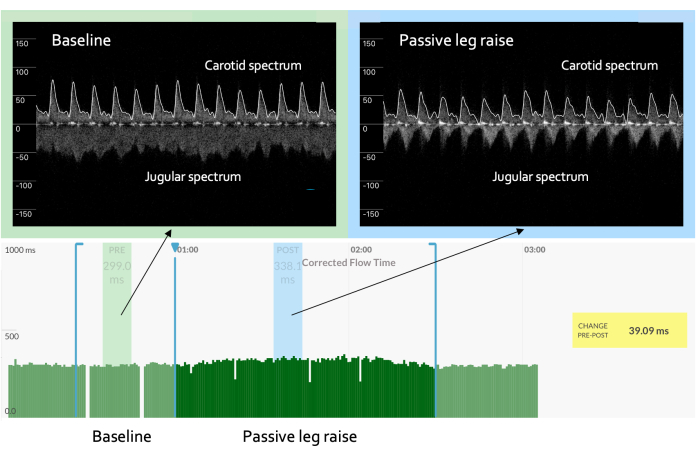
Figure 1: Increased slope of the cardiac function curve. In an example of a "normal" or "expected" result, the venous waveform progresses from being high velocity, low amplitude, and non-pulsatile to being lower velocity, higher amplitude, and pulsatile in character. The pulsatile venous waveform can be marked by a monophasic signal, as seen here. Concomitantly, the arterial Doppler waveform shows an increase in the ccFT from baseline, suggesting that the increase in the cardiac preload is met by a rising cardiac output. These responses, taken together, indicate a "cardiac function" curve with a steep slope. The y-axis on the spectrum represents the velocity in centimeters per second. The positive velocity is toward the brain (e.g., the carotid artery), while the negative velocity is toward the heart (e.g., the jugular velocity). The x-axis on the spectrum is time. Please click here to view a larger version of this figure.
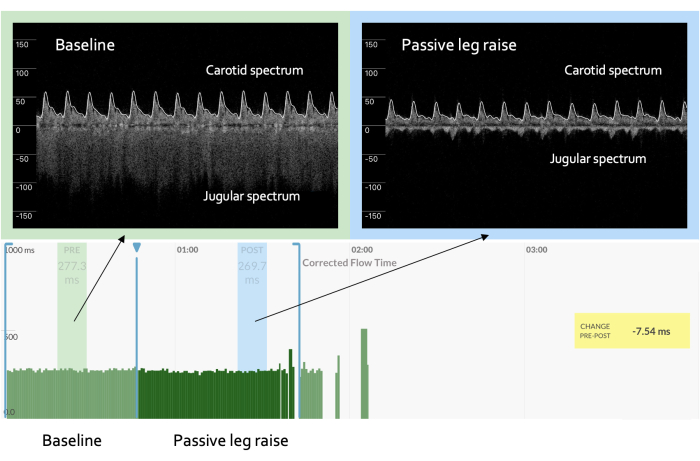
Figure 2: Flattened slope of the cardiac function curve. An "abnormal" response during a preload challenge is marked by a venous Doppler waveform that evolves as above but with an arterial response that reveals no significant change or even a decrease in the ccFT as compared to baseline, as seen here. This constellation of venous and arterial findings implies a flat or, potentially, impaired cardiac function curve with increased preload. Please click here to view a larger version of this figure.
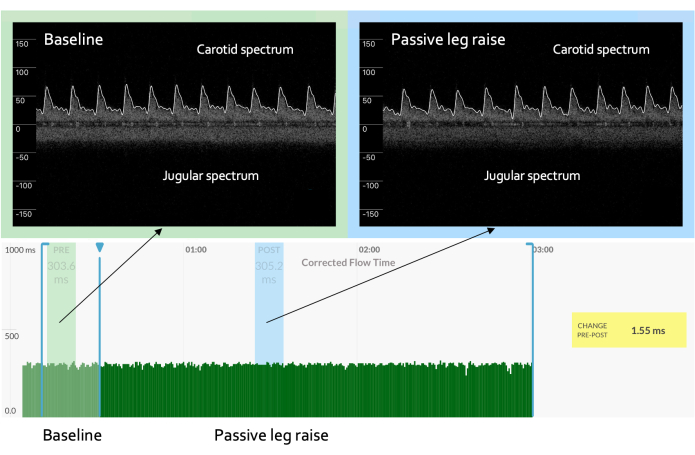
Figure 3: No change in the venous Doppler. A preload challenge that shows no significant change in the venous Doppler waveform could represent an inadequate change in cardiac filling, meaning no change in the arterial spectrum is expected. Please click here to view a larger version of this figure.
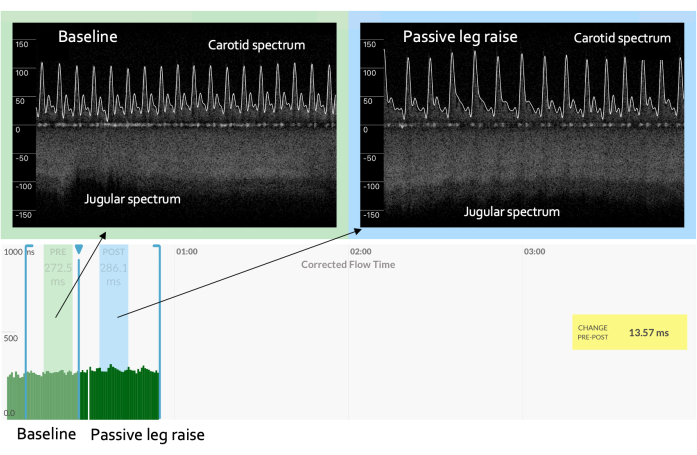
Figure 4: Falling preload during a preload challenge. A preload challenge that shows rising venous velocity and a significant increase in arterial Doppler measures may mean augmented adrenergic tone (i.e., sympathetic stimulation) such that the cardiac function increases independently of the venous return. This circumstance could be the result of a "non-passive" leg raise, for example, if the patient strains to change their body position. Please click here to view a larger version of this figure.

Figure 5: The device on a volunteer. Please click here to view a larger version of this figure.
