This paper aims to provide significant ultrasound parameters that are predictive of a difficult laryngoscopy. To date, 30 studies have analyzed several different ultrasound parameters. Two meta-analyses have identified the five most studied parameters that significantly differ between easy and difficult direct laryngoscopy views and have higher sensitivity and specificity than the classic Mallampatti classification12. This narrative review follows the scanning protocols from the studies shown in Table 1 and Table 2.
Distance from the skin to the epiglottis (DSE)
To obtain the DSE at the level of the thyroid membrane, the patient is placed supine, with the head and neck in a neutral position and without a pillow. The transducer is placed transversely along the anterior surface of the neck and is moved from the floor of the mouth to the sternal notch level. The epiglottis is a hypoechoic (dark) curvilinear structure visualized via the thyroid membrane anteriorly and the bright air-mucosa interface posteriorly. The transducer tail is slightly angled cephalad or/and caudal for optimal visualization. Swallowing enables a mobile view of the epiglottis. The measurements are from the skin to the posterior border of the epiglottis along the central axis and 1 cm to the left and right and are averaged.
A recent meta-analysis by Carsetti et al. of 15 eligible studies found the distance from the skin to the epiglottis (DSE) was the parameter that correlated the most with a difficult direct laryngoscopy12. The DSE was higher in patients with a higher Cormack-Lehane laryngoscopy grade. The average DSE ultrasound measurement was >2-2.5 cm, with a positive predictive value (PPV) of 30%-49.4%, indicating a 30%-50% probability of difficult intubation. The negative predictive value (NPV) ranged from 95%-97%, meaning the likelihood of easy intubation with the above ultrasound parameter would be 95%-97%. In clinical practice, a positive result prompts caution in the intubation method12.
Hyomental distance (HMD) and hyomental distance ratio (HMDR)
The HMD is determined by obtaining a submandibular image, which involves placing the transducer in the sagittal plane – longitudinally – in the submental space along the long central axis of the body. The image of the floor of the mouth shows a fine tissue echogenicity between the acoustic shadows of the mentum and the hyoid bone. The hard palate projects a hyperechoic white line. The HMD is measured from the upper border of the hyoid bone to the lower edge of the mentum of the mandible. The HMDR is the ratio of the hyomental distances in the neutral head position and the extended head position. The HMDR reflects the ability to estimate the submandibular space, which is essential during laryngoscopy. The hyoid bone moves with the extension of the neck, increasing the submandibular area. The inability to visualize the hyoid bone on ultrasound increases the likelihood of a difficult direct laryngoscopy. The below parameters are associated with a difficult direct laryngoscopy and are predictive in both the obese and general populations13,14:
1. HMD in the neutral position in the range of 3.43-4.55 cm (sensitivity: 100%, specificity: 71.4%)
2. HMD in the extended head position less than 5.50 cm (sensitivity: 100%, specificity: 71.4%)
3.HMDR less than 1.20 cm (sensitivity: 75%, specificity: 76.2%)
Distance from the skin to the vocal cords (SVC)
Placing the ultrasound transducer on the thyroid cartilage in the transverse position allows the vocal cords to be visualized within a large upside-down V-shaped structure. The vocal cords display fine tissue echogenicity. With age, the thyroid cartilage calcifies at the level of the vocal cords. The vocal cords move with respiration. They are hypoechoic and triangular in shape, overlie the vocal cord muscles, and are medially attached to the hyperechoic ligaments; with phonation, the vocal cords close at the midline. The false vocal cords are hyperechoic because they contain fat, are parallel and cephalad, and do not move during phonation. Fine movements of the transducer cephalad and caudad distinguish the true vocal cords from the false vocal cords. The false vocal cords are hyperechoic, more prominent, and circular to oval. The true vocal cords are often only distinguished by the hyperechoic vocal cord ligaments.
A study by Ezri reported an overall 0.27 cm higher SVC value in difficult direct laryngoscopy and SVC measurements from 1.10-2.80 cm. The sensitivity and specificity were 53% and 66%, respectively10. A second study noted a distance between 0.92-1.30 cm with greater than 0.38 cm difference and a sensitivity and specificity of 75% and 80.6%, respectively, correlating with a difficult laryngoscopy11,15.
Distance from the skin to the hyoid bone (SHB)
The placement of the probe transversally over the hyoid bone optimizes the view. The hyoid bone is a bright echogenic line that is curved upside. Below it, there is a hypoechoic shadow.
A distance of greater than 1.28 cm from the skin to the hyoid bone correlates with difficult direct laryngoscopy. The sensitivity is 85.7%, and the specificity 85.1%. In addition, a difference of 0.2 cm differentiates an easy airway from a difficult airway. In contrast, the Mallampatti airway classification is inconsistent, less sensitive, and less specific12. The ability to visualize the hyoid bone is associated with a lower Cormack-Lehane laryngoscopy grade and easy intubation13.
Thyrohyoid membrane (THM)
The thyrohyoid membrane expands from the caudal border of the hyoid bone to the cephalad border of the thyroid cartilage. The view is optimized with the transducer in the transverse position between these two structures. The epiglottis is a hypoechoic (dark) curvilinear structure at this level. The thyrohyoid membrane distance is measured from the skin to the anterior border of the epiglottic space.
Adhikari et al. and Pinto et al. found that the anterior neck soft tissue thickness at the thyrohyoid membrane level is an independent predictor of difficult laryngoscopy8,16. Compared to an easy direct laryngoscopy, a 0.24 cm lower THM value was statistically significant for a difficult direct laryngoscopy. A value of more than 2.8 cm was predictive of a difficult laryngoscopy. Adhikari et al. did not report the sensitivity or specificity8. In the study from Pinto et al.16, the sensitivity was 64.7%, and the specificity was 77.1%. These two studies did not find an association between ultrasound measurements and clinical evaluation. Still, they concluded that the ultrasound measurement at the level of the THM was a better predictor than the SVC measurements.
Two other parameters are often mentioned in the ultrasound evaluation of the airway: the distance from the skin to the anterior surface of the first tracheal cartilage and the thickness of the tongue. However, these parameters were identified by small studies with inconsistent results, and a larger sample size is needed to supply substantial evidence17.
Table 1: Ultrasound parameters associated with difficult direct laryngoscopy. Please click here to download this Table.
Table 2: Ultrasound parameters in a difficult airway. Please click here to download this Table.
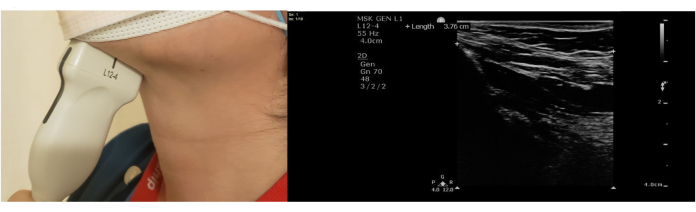
Figure 1: Hyomental distance (HMD). Please click here to view a larger version of this figure.
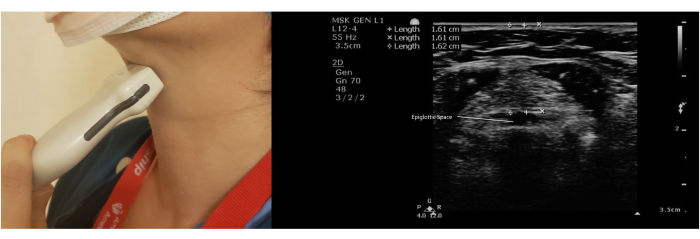
Figure 2: Thyrohyoid membrane (THM). Please click here to view a larger version of this figure.
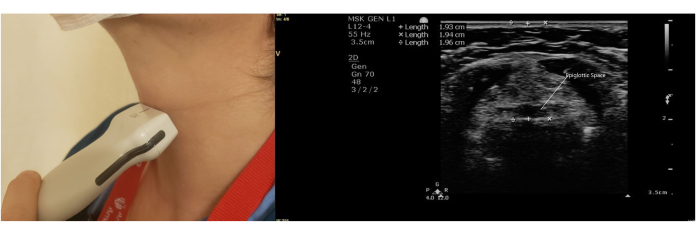
Figure 3: Distance from the skin to the epiglottis (DSE). Please click here to view a larger version of this figure.
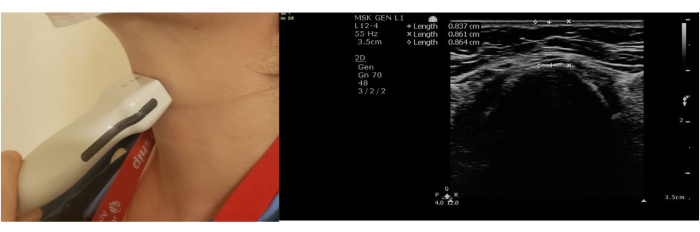
Figure 4: Distance from the skin to the hyoid bone (SHB). Please click here to view a larger version of this figure.
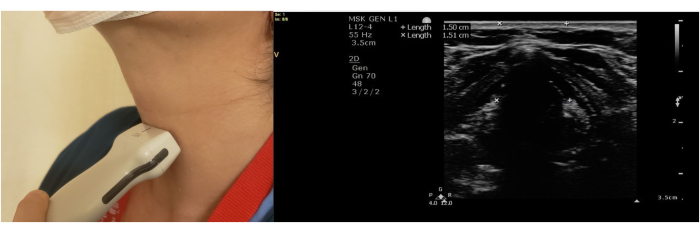
Figure 5: Distance from the skin to the vocal cords (SVC). Please click here to view a larger version of this figure.
