The whole setup includes a syringe pump, a syringe, and a microfluidic chip. The cell suspension in the syringe is connected to the syringe pump, and the cell suspension is introduced into the microfluidic chip to capture the cells. The capture efficiency for all the microfluidic chips utilized was around 90% or above. For the wave chip, we designed microstructures with varied gaps. The small gaps are used to capture the CTCs, and the big gaps are used to accelerate the flow rate. The cell suspension flows quickly in the big gap areas. The missed CTCs tend to be captured by the small gaps in the subsequent array16. For ellipse chips, we designed line-line gaps instead of point-point gaps to form a slim tunnel to enhance the capture. Therefore, high capture efficiency was achieved1. We designed an ellipse structure to avoid edges and corners to maintain viability. The trapezoid filters have two circular spiral channels with embedded trapezoid and circular micropost barriers. For trapezoid filters, the capture efficiencies for MCF-7, MDA-MB-231, and HeLa were 94%, 95%, and 93%, respectively18.
Figure 1 shows that all the tumor cells were captured by the wave chip. Since all the tumor cells were concentrated around the wave micropost array, this indicates high capture efficiency for this microfluidic chip, as demonstrated by the number of tumor cells that were captured. Therefore, this setup makes it much easier to capture rare tumor cells; indeed, the chip is fabricated to capture a large number of tumor cells as well as rare number of tumor cells. For example, if the chip is solid or reproducible enough to capture 10,000 tumor cells, it is easy for the chip to capture 10-100 cells. Video 1 shows how rare number of tumor cells were obtained for the pre-experiment. A hollow needle made using a micropipette puller was used to aspirate 1, 2, 3, 4, 5, 6, 7, 8, 9, and 10 tumor cells from a culture dish with diluted tumor cells stained with calcein AM in PBS. The cells were absorbed by the silica gel tube connected with the hollow needle. A tumor cell with green immunofluorescence was suctioned into the hollow needle. Blowing into the hollow tube led to the tumor cell inside the hollow needle being discharged into a microcentrifuge tube1. This is the procedure to obtain rare tumor cells. Figure 2 shows CTCs from a gastric cancer patient captured using small-ellipse microfilters. Figure 3 shows the CTCs from a colorectal cancer patient captured using trapezoid microfilters and emitting both blue and green fluorescence. Figure 4 shows tumor cells grown on the chip after capture, which are ready to be treated with anti-cancer medicine. These findings illustrate that big-ellipse microfilters do not have any negative effects on cell viability.
Figure 5 shows the clinical immunofluorescence analysis of colorectal CTCs captured on the microfluidic chip. These are seen in brightfield and stained with Hoechst, CK-FITC, and CD45-PE staining. The CTCs were recognized as DAPI+/CK+/CD45−, and the WBCs were identified as DAPI+/CK−/CD45+. Figure 6 shows colorectal tumor cells cultured on the big-ellipse chip after capture. Figure 7 shows colorectal tumor cells captured on the big-ellipse microfilters. Clinically, CTCs in patient blood were captured by wave chips, trapezoid microfilters, and big-ellipse microfilters, indicating that these three chips are successful in capturing CTCs. Potentially, they could be applied in CTC products, such as CTC isolation products, with high efficiency.
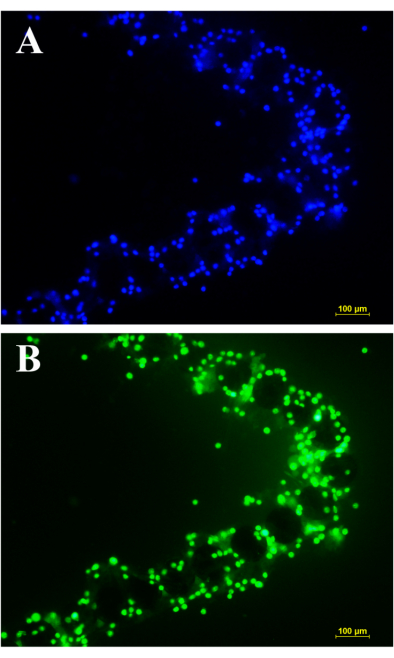
Figure 1: Wave chip capture. All the tumor cells of MCF-7 were captured around the array of the wave chip without any cells missing. Since there were not any tumor cells in any other area besides the array, this indicates the high capture efficiency of the chip. A large number of tumor cells were captured. Therefore, rare tumor cells can also be easily captured. Tumor cells of MCF-7 were captured by wave chip and (A) stained with Hoechst and (B) stained with calcein AM. Scale bar: 100 µm. Please click here to view a larger version of this figure.
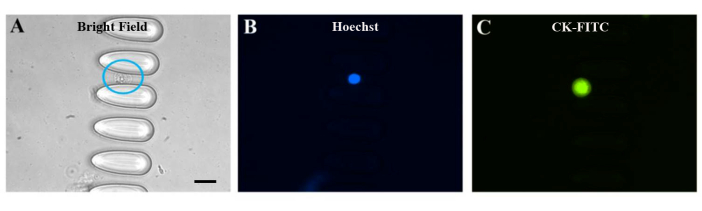
Figure 2: Clinical sample for CTCs captured by small-ellipse microfilters. Clinical CTCs of a gastric cancer patient captured by small-ellipse microfilters. The CTCs were identified in brightfield and with both blue and green fluorescence. The blue circle in (A) indicates a CTC of a gastric cancer patient captured inside the chip. From the images taken, it can be seen that there were no other cells in any other areas, indicating that the capture purity was high for this chip. Tumor cells of MCF-7 were captured by small-ellipse microfilters and seen in (A) brightfield, (B) stained with Hoechst, and (C) stained with CK-FITC. Scale bar: 20 µm. Please click here to view a larger version of this figure.
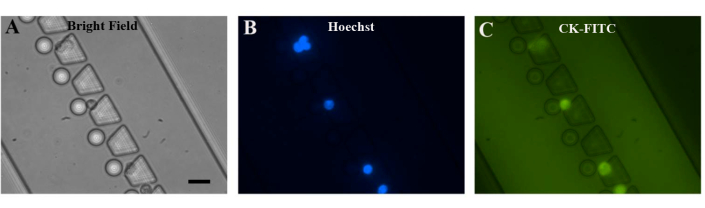
Figure 3: Clinical sample of CTCs captured by trapezoid microfilters. Clinical CTCs from a colorectal cancer patient were captured by trapezoid microfilters. In these images, it can be seen that six CTCs were captured, indicating that the capture efficiency was high in the small field. Additionally, no other cells appeared, indicating that the capture purity was extremely high for this chip. Tumor cells of MCF-7 were captured by trapezoid microfilters and seen in (A) brightfield, (B) stained with Hoechst, and (C) stained with CK-FITC. Scale bar: 20 µm Please click here to view a larger version of this figure.
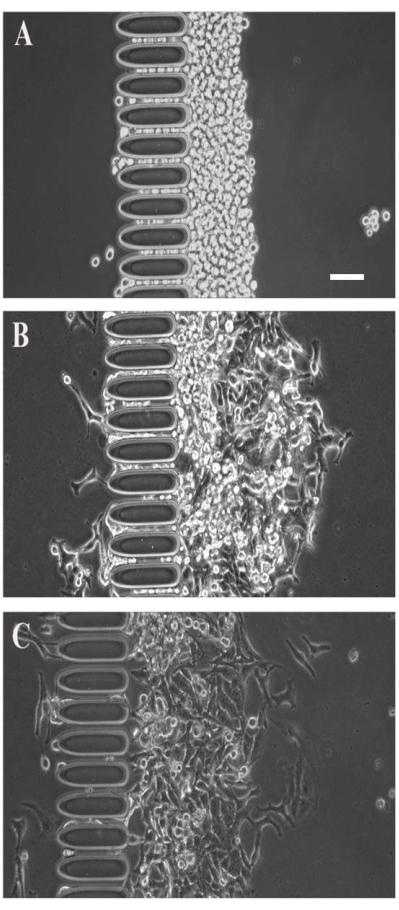
Figure 4: Culture of CTCs captured by big-ellipse microfilters. Tumor cells of MCF-7 were captured by big-ellipse microfilters in front of a big-ellipse micropost array. No tumor cells passed through the array, indicating high capture efficiency for this chip. After capture, the tumor cells grew for 24-48 h. This indicates that both the capture efficiency and viability were very high for the big-ellipse microfilters. The cultured tumor cells of MCF-7 were captured by big-ellipse microfilters and seen at (A) 0 h after capture, (B) 24 h after capture, and (C) 48 h after capture. Scale bar: 50 µm. Please click here to view a larger version of this figure.
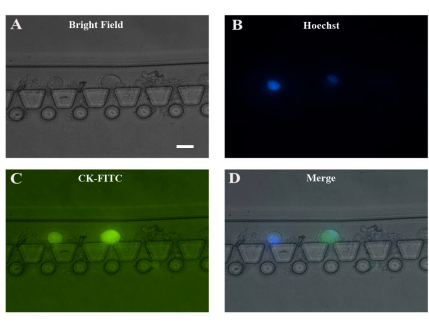
Figure 5: Example of a clinical sample used for CTC capture by trapezoid microfilters. Clinical CTCs from a colorectal cancer patient were captured by trapezoid microfilters. In these images, it can be seen that two CTCs were captured, indicating high capture efficiency. There was no other cell disturbance except residues of RBCs in the chip. Thus, for the clinical pre-processing of CTC capture, it is better not to use red blood cell lysis. CTCs of colorectal cancer were captured by trapezoid microfilters and seen in (A) brightfield, (B) stained with Hoechst, (C) stained with CK-FITC, and (D) seen in merged images. Scale bar: 20 µm. Please click here to view a larger version of this figure.
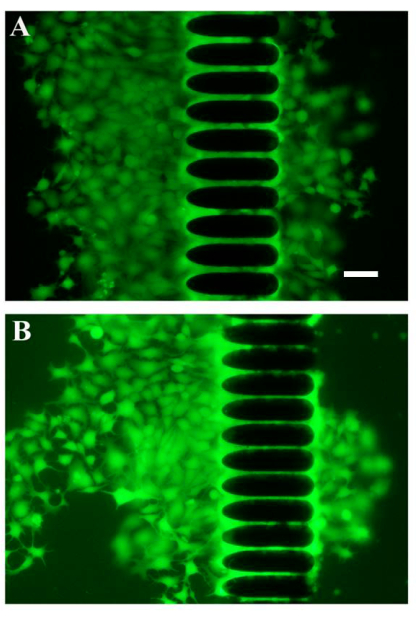
Figure 6: Example of cultured CTCs captured by a big-ellipse chip. Tumor cell cultures of MCF-7 cells in front of the big-ellipse micropost array and behind the big-ellipse microfilters. The tumor cells stained with calcein AM emitting green fluorescence grew as desired, indicating that the cell viability for this chip was very high. In total, there were 15 arrays, with varied gaps for each array organized by big-ellipse microposts. MCF-7 tumor cells were cultured on the big-ellipse chip after capture (A) in one array and (B) in another array. Scale bar: 50 µm. Please click here to view a larger version of this figure.
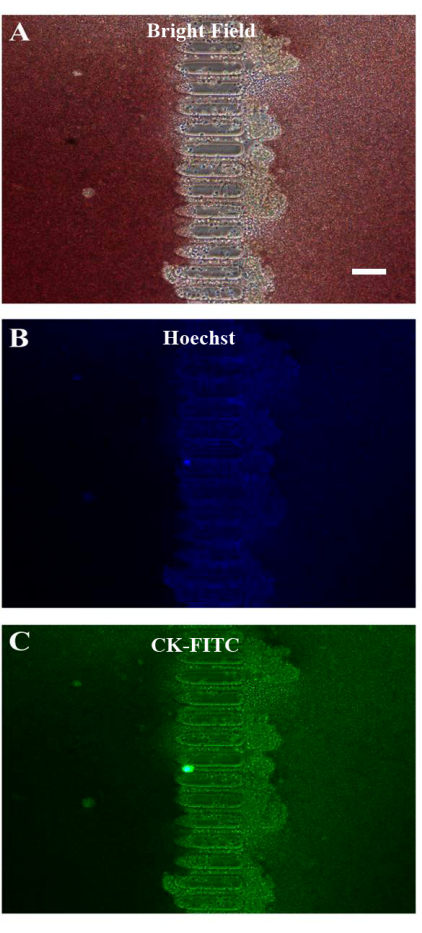
Figure 7: Example of a clinical sample used for CTC capture by big-ellipse microfilters. Clinical CTCs from a colorectal cancer patient were captured by big-ellipse microfilters. From the images, it can be seen that there was RBC contamination. This indicates that the whole patient blood sample must be diluted and that the chip needs to be flushed after capture. CTCs of clinical colorectal cancer patient blood samples were captured on the big-ellipse chip and seen in (A) brightfield, (B) stained with Hoechst, and (C) stained with CK-FITC. Scale bar: 100 µm. Please click here to view a larger version of this figure.
