The protocol was approved by The Norwegian Food Safety Authority (approval nr. 25030), and the experiments were conducted according to European, Norwegian, and Institutional regulations. The replication of this model requires obtaining ethical approval for the animal experiments in line with institutional and national regulations and ensuring to conduct the experiments according to the three Rs23. All personnel handling the animals need to be certified with functions A, B, and D in accordance with Article 23 and Article 24 of the EU Directive 2010/63/EU24, or equivalent. Carefully monitor the animals during the whole experiment, and adjust the anesthesia, ventilator settings, temperature, and animal positioning to ensure the animals' well-being. Critically assess the model and its application regularly, and refine as required and possible.
NOTE: The piglets used in this study were aged 12-36 h, weighed 1.7-2.3 kg, had equal gender distribution, were of mixed Norwegian Landrace, Duroc, and Yorkshire race, and were genetically unmodified. Step 1 and step 2 of the protocol include general anesthesia and data sampling procedures that apply throughout the experiment, and steps 3-10 detail the experimental procedures, including the preparation of the animals, surgical intervention, asphyxiation until cardiac arrest, resuscitation, and post-resuscitation observation.
1. Anesthesia protocol (TIME: applies to the whole experiment)
- Induce anesthesia with a bolus of IV fentanyl (50 µg/kg) and pentobarbital (15-20 mg/kg) in a peripheral venous catheter in an ear vein.
CAUTION: Fentanyl is harmful if inhaled or ingested and irritates the eyes and skin. It is also a restricted drug. Its supply and use should be monitored and regulated according to regulations for restricted drugs. Pentobarbital is harmful if ingested and irritates the eyes and skin. - Maintain anesthesia with IV fentanyl (50 µg/kg/h) until asphyxiation, and then stop during asphyxia, and reinstitute at 25 µg/kg/h after the return of spontaneous circulation (ROSC).
NOTE: The high-dose fentanyl anesthesia used in this model stems from tens of years of refining the model in a collaborative effort involving neonatologists and pediatric anesthesiologists. High-dose fentanyl anesthesia is associated with cardiovascular and hemodynamic stability25,26 in human adults and neonates. However, one study in newborn piglets showed that fentanyl use was associated with reduced HR and cardiac output (CO) and increased mean arterial pressure (MAP), left ventricular end-diastolic pressure, and total peripheral resistance index27. - Monitor the piglet's well-being throughout the whole experiment. Check the muscle tone and assess the vitals to make sure the piglet is thoroughly anesthetized. If the piglet shows signs of distress, administer additional IV fentanyl or IV pentobarbital according to clinical judgment.
2. Data sampling and registrations (TIME: applies to the whole experiment)
- Print a paper case registration form (CRF) for each piglet. The CRF contains information about the HR, BP (including MAP), oxygen saturation (SpO2), regional cerebral oxygen saturation (NIRS), temperature, extra medication provided, and shivering.
- On the CRF, give the piglet an ID number, and record the piglet's weight and gender on the front page.
- Make the registrations every 5 min during the stabilization period and just before the induction of asphyxia. After the induction of asphyxia, make the first registration after 10 min and then every 5 min until cardiac arrest. If ROSC is achieved, make the registrations as soon as possible after ROSC, every 5 min for the first hour post ROSC, and then every 30 min for the rest of the observation period.
- On the CRF, state when to collect the different specimens.
- Collect full blood and plasma at the start of the stabilization, just before the induction of asphyxia, at cardiac arrest, at ROSC, 30 min, 60 min, 120 min, 240 min, and 540 min post ROSC, and at the end of the study (570 min).
NOTE: It is important to calculate how much blood can be drawn from each piglet. As an example, less blood can be drawn from smaller piglets, unstable piglets, and piglets that have suffered some blood loss from the neck surgery. It is also vital to watch the hemoglobin (Hb) from the acid-base status throughout the experiment. In this study, piglets with Hb <6 g/dL were excluded. - Collect urine at 240 min post ROSC and at end of the study (570 min).
- Take the acid-base status at the start of the stabilization, just before the induction of asphyxia, 10 min after the induction of asphyxia, and then every 5 min until cardiac arrest. Take the acid-base status at cardiac arrest, at ROSC, 5 min, 15 min, 30 min, 60 min, 120 min, 240 min, and 540 min post ROSC, and at the end of the study (570 min).
- Collect cerebrospinal fluid (CSF) at the end of the study (570 min).
- Collect full blood and plasma at the start of the stabilization, just before the induction of asphyxia, at cardiac arrest, at ROSC, 30 min, 60 min, 120 min, 240 min, and 540 min post ROSC, and at the end of the study (570 min).
- Collect full blood and plasma from the central arterial catheter.
- Withdraw 2 mL of blood from the central arterial catheter into a heparinized syringe, and put to the side.
- Then, withdraw 2.5 mL of blood into a new heparinized syringe. Place 0.5 mL of the last drawn full blood in a microcentrifuge tube, and snap-freeze in liquid nitrogen.
- Place the remaining 2 mL in an appropriately sized EDTA vial, and centrifuge at 1,700 x g at 4 °C for 10 min. Pipette the plasma (which separates from the buffy coat and erythrocytes as the top layer) into microcentrifuge tubes, and snap-freeze in liquid nitrogen.
- Withdraw another 0.2 mL of blood from the central arterial catheter into a new heparinized syringe. Place the syringe in the acid-base machine (see Table of Materials), and fill in the relevant information (the ID, time point, and the piglet's temperature).
- Push the blood that was withdrawn into the first heparinized syringe back into the arterial catheter. Flush the arterial catheter with heparinized normal saline to ensure that all of the blood is returned to the piglet's circulation.
- Collect urine by suprapubic aspiration of urine.
- Locate the landmarks: the area between the third-lowest and second-lowest pairs of nipples, approximately 2 cm below the umbilicus, and a few millimeters lateral to the midline.
- Use a 10 mL syringe with a 23 G cannula. Advance the cannula vertically approximately 1 cm, and aspirate until the syringe fills with urine. Put the urine in a cryogenic tube, and snap-freeze in liquid nitrogen.
- Collect CSF by a lumbar puncture.
- Place the piglet on its side, and draw the hindlimbs up toward the chest. Locate the landmarks: between the spinal tags at the level of the piglet's iliac crest.
- Advance a 21 G cannula slightly cranially between the spinal tags until the CSF emerges. Put the CSF in microcentrifuge tubes, and snap-freeze in liquid nitrogen.
- Collect continuous ECG and invasive arterial BP data (see step 6 and step 7) using a data acquisition and analysis software (see Table of Materials). Perform NIRS (see step 7) with a commercially available NIRS machine (see Table of Materials).
3. Preparation (TIME: weeks to months, as long as needed)
- Obtain ethical approval for the animal experiments.
- Contact a farmer, and organize the selection of piglets (age: 12-36 h, equal gender distribution, weight: 1.7-2.3 kg), delivery date, and transportation arrangements.
NOTE: Selecting piglets from the same race (in this study, a mix of Norwegian Landrace, Duroc, and Yorkshire) and farm, ideally from the same litter and within a narrow age range, is important for reducing biological and physiological variance. - Make sure personnel are available at the set date(s).
- Check that all the necessary equipment is available and that all the instruments and observation tools are working. Check the expiry date of the asphyxia gas (8% O2, 92% N2) and that it is not empty.
- Set up the lab and all the equipment so that it is ready for the reception of the piglets. Calibrate all the necessary equipment.
- Perform sample size estimation in the case of a randomized controlled trial, and prepare the randomization of the piglets.
4. Reception of piglets (TIME: from 10 min to 2 h, depending on the number of piglets)
- Organize the transport of the domestic piglets from the farm to the surgical facility on the day of the experiments. Cover the container "floor" with fine wood chips and hot water bottles to maintain the piglets' temperature. Make burr holes in the container to ensure the circulation of air.
- Obtain information from the farmer about the age and weight of the piglets. Verify their weight upon arrival.
- Measure the SpO2 and HR by placing a pulse oximeter (PO) probe (see Table of Materials) on the piglet's hindlimb while the piglet is calm and at ease in the container.
- Prepare all the instruments, and turn on the heat on the electric heating mattresses on the surgical table.
- Let the piglets rest in the container until everyone in the team is ready for the induction of anesthesia and surgical intervention.
5. Induction of anesthesia, intubation, and mechanical ventilation (TIME: 15 min)
- Prepare the equipment for IV access and intubation.
- Apply the PO probe on a hindlimb for the monitoring of oxygenation and HR during the induction of anesthesia and intubation.
- Ensure that person one holds the swaddled piglet still and calm. Ensure that person two inserts a peripheral intravenous catheter into an ear vein. Flush the catheter with approximately 1 mL of normal saline to confirm placement. Secure the catheter with tape.
- Inject a bolus dose of fentanyl and pentobarbital into the ear vein (as described in step 1.1). Flush the catheter with 1 mL of normal saline. Check that the piglet is anesthetized by assessing the withdrawal reflexes.
- Ensure that person one places the piglet in the supine position. Open the mouth, and pull the tongue out with a 10 cm x 10 cm gauze swab. Keep the larynx in a straight line.
- Ensure that person two uses the laryngoscope (see Table of Materials) to lift the tongue. Advance the laryngoscope to lift the epiglottis and visualize the vocal cords. Advance the endotracheal tube (ETT, see Table of Materials) through the vocal cords.
NOTE: Using a cuffed ETT may make the advancement of the ETT through the vocal cords more challenging. If intubation is difficult, it is particularly important to watch the piglet's vital signs. If the vitals drop, place a mask over the piglet's snout, connect the mask to a self-inflating bag, and manually ventilate the piglet until the vitals normalize. Then, try intubating again. If it is still challenging, consider giving an extra dose of pentobarbital. In rare cases (e.g., upper airway anomaly), a tracheostomy should be done. However, with experienced staff, intubation is usually easily performed. - Connect the ETT to a self-inflating bag (see Table of Materials), and start the manual ventilation.
- Confirm correct ETT placement by 1) bilateral and symmetric chest rise upon ventilation, 2) bilateral and symmetric breath sounds over the lung fields with no sound of air entry over the epigastrium, 3) SpO2 and HR responses, and 4) condensation inside the ETT. The expired CO2 could also be measured (semi)quantitatively if in doubt.
- Inflate the ETT cuff. Secure the ETT at a depth of 12-13 cm (for a 2 kg piglet) with tape that has been split longitudinally in half. Drape the tape around the part of the ETT immediately distal to the front teeth, and continue around the snout.
- Continue to manually ventilate the piglet until it is transferred to the surgical intervention table where it is connected to a mechanical ventilator. On the table, connect the ETT to the mechanical ventilator (see Table of Materials) with the following settings: PInsp = 15-20 cm H2O, Peep = 5.0 cm H2O, FlowInsp = 8.0 L/min, Frequency = 30 bpm, and TInsp = 0.34 s.
NOTE: If the piglet has SpO2 <90%, the PInsp and Frequency may be increased until the SpO2 is ≥90%. Supplemental oxygen could be used if the resuscitation protocol does not involve the comparison of different FiO2s. - Place a rectal thermometer, and secure it with surgical tape around the piglet's tail.
- Maintain the piglet's temperature (38.5-39.0 °C) with warm blankets/towels draped around the piglet like a nest, by adjusting the temperature of the heating mattress under the piglet, and/or by filling rubber/latex gloves with hot tap water and placing them in the towels surrounding the piglet. Watch the temperature of the piglet during the surgical intervention, and perform temperature-stabilizing measures as needed.
6. Surgical intervention (TIME: 20 min)
- Prepare all the necessary equipment, and fill all the catheters with normal saline (Figure 1). Write down the time the surgical intervention starts on the CRF.
- Sterilize the skin of the anesthetized piglet with 5 mg/mL colored chlorhexidine using 3-5 surgical sponges.
- Make a 2.5 cm long skin incision on the right side of the piglet's neck using a scalpel.
- Use eyelid retractors to retract the skin on both sides of the incision.
- Use artery forceps to dissect and expose the internal jugular vein (Figure 2).
- Place two nylon 3-0 suture threads under the jugular vein to keep it stable.
- Hold one of the sutures in one hand and the central venous catheter in the other (Figure 3). Insert the central venous catheter, and withdraw the needle.
- Tie one of the suture threads that was used to hold the vein around the vein (and the catheter) in the area where the catheter is inside the vein (Figure 4).
NOTE: Make sure that the holding suture is not tied too tightly around the catheter and that the knot is proximal to the distal tip of the catheter. - Flush with 1 mL of normal saline to confirm the correct placement of the catheter.
- Close the skin with absorbable 4-0 sutures.
- Connect fentanyl 50 µg/kg/h and a balanced carbohydrate-electrolyte solution (10 mg/mL glucose, see Table of Materials) to the central venous catheter.
- Make a 2.5 cm long skin incision on the left side of the piglet's neck using a scalpel. Make the incision slightly more medial than the incision on the right side of the neck.
- Use eyelid retractors to retract the skin on both sides of the incision.
- Then, use artery forceps to dissect and expose the common carotid artery (medial to the sternocleidomastoid muscle).
- Place two nylon 3-0 suture threads under the common carotid artery to keep it stable.
- Hold one of the sutures in one hand and the central arterial catheter in the other. Insert the central arterial catheter, and withdraw the needle.
- Tie one of the suture threads that was used to hold the artery around the artery (and the catheter) in the area where the catheter is inside the artery.
NOTE: Make sure that the holding suture is not tied too tightly around the catheter and that the knot is proximal to the distal tip of the catheter. - Flush with 1 mL of normal saline to confirm the correct placement of the catheter.
- Use absorbable 4-0 sutures to secure the catheter wings to the skin and close the skin.
- Connect to invasive arterial BP monitoring (see Table of Materials), and start recording using the data acquisition and analysis software.
NOTE: Make sure that the invasive arterial BP transducer is calibrated at the heart level to get correct BP readings. - Cover with a transparent dressing. Now, the central arterial catheter is in place.
- Write down on the CRF the time the surgery ended.
7. Stabilization (TIME: Minimum 1 h, but as long as needed to stabilize the piglet following surgery and for staff to prepare for the induction of asphyxia)
- Connect the piglet to the ECG monitoring equipment (see Table of Materials).
- Shave and remove the hair as necessary before placing the electrodes. Place two electrodes on each side of the thorax-on the medial side of each upper limb. Place the third electrode on the left side of the umbilicus.
- Connect the leads to the electrodes, and start recording using the data acquisition and analysis software.
- Connect the piglet to a non-invasive CO monitoring device (see Table of Materials).
- Shave and remove the hair as necessary before placing the electrodes (see Table of Materials). Place the first electrode on top of the piglet's head, just behind the eyes, the second on the left side of the neck, the third on the left side of the abdomen, midaxillary at the level of the umbilicus, and the fourth electrode on the left thigh.
- Fill in the relevant information on the device, and start recording. Due to limited internal memory, adjust the sampling rate according to the duration of the experiment.
- Connect the piglet to NIRS monitoring.
- Shave and remove the hair as necessary before placing the electrodes. Place the NIRS electrodes (see Table of Materials) on the top of the piglet's head, behind the non-invasive CO electrode, and secure with non-transparent tape to protect from light.
- Connect the piglet to additional monitoring equipment if applicable, and perform echocardiography if this is part of the experimental protocol.
- Place the piglet in a comfortable position, preferably prone.
- Conduct the measurements and registrations, and record on the CRF during the stabilization period (see step 2).
- Observe the piglet with regard to temperature, SpO2, HR, BP, and shivering during the stabilization period. Adjust mechanical ventilator settings and the piglet's temperature, and give extra anesthesia as appropriate.
8. Induction of asphyxia and cardiac arrest (TIME: 15-60 min, varies between piglets)
NOTE: All personnel involved need to know their roles before the induction of asphyxia.
- Decide on a time to start the asphyxia (based on the duration of stabilization and availability of personnel), and write this down on the CRF.
- Write down the physiological measurements of the piglet on the CRF, and take blood samples just before the induction of asphyxia.
- Stop the fentanyl IV right before the start of asphyxia.
- To start the asphyxia, turn the oxygen dial on the mechanical ventilator to 100%, and switch the oxygen hose on the ventilator to the asphyxia gas (8% O2, 92% N2).
- Reduce the ventilator rate by 10 inflations/min.
- Make sure the piglet's SpO2 is dropping to ascertain that the induction is successful.
- After 10 min of asphyxia, reduce the ventilator rate by another 10 inflations/min.
- After 10 min of asphyxia, and thereafter every 5 min, take the acid-base status, and write down the physiological measurements of the piglet on the CRF. Continue until cardiac arrest.
- After 20 min of asphyxia, reduce the ventilator rate by another 10 inflations/min.
- After 30 min of asphyxia, clamp the ETT with arterial forceps.
- When the MAP drops below 20 mm Hg, start the continuous auscultation of the heart.
NOTE: Cardiac arrest is defined as a non-audible heartbeat by auscultation and/or the loss of arterial line pulsation. Note that pulseless electrical activity (PEA) on the ECG may occur. - Ensure that person one auscultates the heart. Call out loud when the heartbeat is not audible anymore (cardiac arrest) while removing the ETT clamp. Ensure that person two switches the asphyxia gas hose on the ventilator back to the oxygen outlet. Record the time of cardiac arrest on the CRF, and start a timer.
- Set the FiO2 as assigned by protocol (in this study, the piglets were randomized to receive a FiO2 of 0.21 or 1.0). Set the ventilator settings as follows: PInsp = 30 cm H2O, Peep = 5.0 cm H2O, FlowInsp = 8.0 L/min, Frequency = 40 bpm, and TInsp = 0.34 s.
- Draw blood samples from the cardiac arrest time point, as described in step 2.5.
9. Cardiopulmonary resuscitation (CPR) (TIME: 0-15 min)
NOTE: CPR can be conducted according to International Liaison Committee on Resuscitation (ILCOR) guidelines28, with a 3:1 chest compression to ventilation ratio or different ratios of chest compressions to ventilations depending on the aim of the study.
- If using the ILCOR-recommended 3:1 CPR, conduct the following steps.
- Mechanically ventilate the piglet for 30 s after cardiac arrest. Then, start the chest compressions, and aim for a 3:1 chest compression to ventilation ratio.
NOTE: As the ventilator performs the ventilations and not a person, the chest compressions and ventilations may sometimes be simultaneous/uncoordinated. - Compress the chest to a depth of 1/3 of the thoracic anteroposterior diameter, allow full chest recoil, and use the two-thumb encircling hands technique. Aim to generate a systolic arterial pressure ≥20 mm Hg.
- Administer adrenaline (0.02-0.03 mg/kg) IV after 30 s of chest compressions and then every 3 min of CPR (maximum four doses). Flush with 1 mL of normal saline after each adrenaline administration.
- Mechanically ventilate the piglet for 30 s after cardiac arrest. Then, start the chest compressions, and aim for a 3:1 chest compression to ventilation ratio.
- Determine ROSC by observing the arterial BP tracings and ECG, and confirm by cardiac auscultation. The definition of ROSC is a stable, unassisted HR ≥100 bpm.
- Continue the resuscitation efforts until ROSC or for a maximum of 15 min. If CPR is not successful within 15 min, stop resuscitation efforts, state the time of death, and record on the CRF.
- If resuscitation efforts are successful, write down on the CRF the time of ROSC, the duration of CPR in seconds, and the number of adrenaline doses administered.
- Take blood samples and CRF registrations as soon after ROSC as possible, and continue the registrations as described in step 2 for another 9.5 h (570 min).
10. Post-ROSC observation (TIME: 9.5 h)
- Reinstitute fentanyl IV infusion, initially at 25 µg/kg/h, and titrate according to the clinical effects/requirements.
NOTE: During and after asphyxia, the metabolic rate is reduced, hence the lower dose of fentanyl IV. However, some piglets might need higher infusion rates, and thus, it is important to observe the piglet's vitals and reflexes. - Carefully monitor the piglet for 9.5 h. Adjust the mechanical ventilator settings as required to keep the SpO2 ≥90% and maintain normocapnia (temperature-adjusted partial pressure of CO2 (pCO2) of 5-7.5 kPa).
- Maintain the piglet's temperature at 38.5-39.0 °C, and perform temperature-corrective measures as indicated.
NOTE: The piglets tend to get hypothermic during and after asphyxia. - Take samples and CRF registrations at predetermined time points as dictated by the CRF (step 2).
- At 9.5 h of post-ROSC observation, euthanize the piglet (step 11).
NOTE: Some piglets might not survive the whole 9.5 h of post-ROSC observation. If the piglet shows signs of significant distress and a worsening condition, perform euthanasia earlier.
11. Euthanasia (TIME: 10 min)
- Prepare the dissection table with the necessary surgical equipment, vials to store the tissue samples, and liquid nitrogen to snap-freeze the samples.
- Collect the end of study (570 min) samples as described in step 2.
- Administer IV pentobarbital 150 mg/kg. Perform dissection, place the organ samples in marked cryogenic tubes, and snap-freeze in liquid nitrogen. Store one brain-half in formalin if desired.
- Place the samples from the experiment (full blood, plasma, urine, CSF, and organ samples) in a −80 °C freezer, or store in another manner as dictated by the planned analyses.
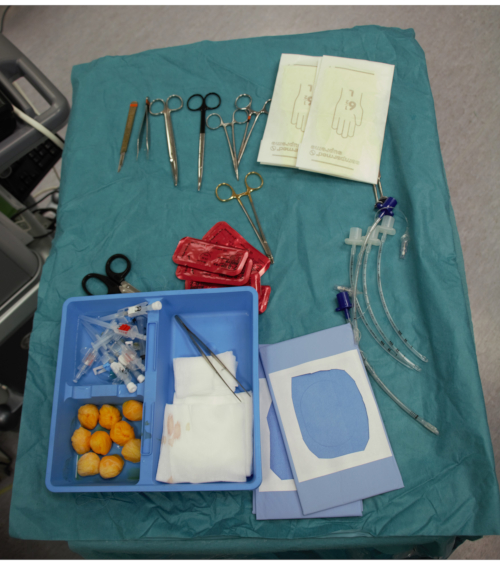
Figure 1: Sterile table with surgical tools. The surgical tools are prepared and stored on a sterile table before the start of the neck surgery. Please click here to view a larger version of this figure.
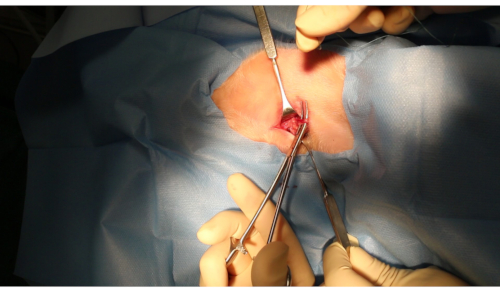
Figure 2: Internal jugular vein. The internal jugular vein after it has been dissected free and exposed. Please click here to view a larger version of this figure.
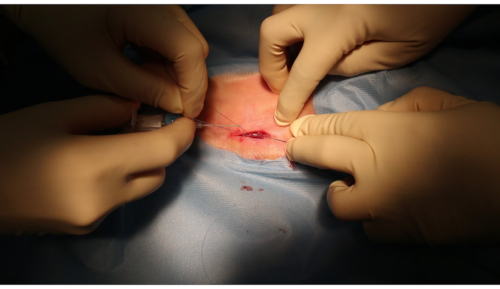
Figure 3: Insertion of the central venous catheter. The suture threads are held just prior to the insertion of the central venous catheter. Please click here to view a larger version of this figure.
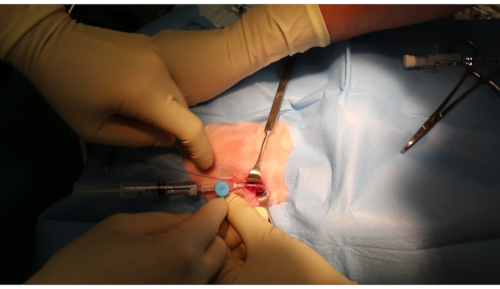
Figure 4: Sutures to secure the central venous catheter. The sutures are tied around the vein (and the catheter) to secure the catheter inside the vein. Please click here to view a larger version of this figure.
After the piglets have been instrumented and stabilized, ECG and BP measurements are continuously collected using a data acquisition and analysis software. The hemodynamic changes during asphyxia can easily be seen in the software (Figure 5). The BP drops gradually during asphyxia until cardiac arrest when the BP = 0. After ROSC is achieved, the BP increases, and then after some time, it normalizes again. The BP and ECG data can be used for different types of analyses, for example, the calculation of coronary perfusion pressure during CPR and changes in BP and ECG rhythm and morphology before, during, and/or after asphyxia.
Cardiac stroke volume and cardiac index are continuously monitored with impedance cardiography (a non-invasive cardiac output measurement)21. To study cardiac injury, myocardial markers of oxidative stress and anaerobic metabolism are measured19. In addition, cardiac enzymes including cardiac troponin T can be measured in the plasma (results not yet published).
The asphyxia changes the piglet's physiology. Figure 6 shows an example of how HR (Figure 6A), MAP (Figure 6B), pH (Figure 6C), pCO2 (Figure 6D), base excess (Figure 6E), and lactate (Figure 6F) change throughout the experiment. As expected, MAP, pH, and base excess decrease during asphyxia, while pCO2 and lactate increase (mixed respiratory and metabolic acidosis). Toward the end of the experiment, the values normalize.
Historically, experiments were performed with tracheostomized piglets11,13,15,16,19 (i.e., with a leak-free airway). To limit surgical stress, the piglets were endotracheally intubated with uncuffed ETTs in experiments from 2019. In those experiments21, notably lower ROSC rates were observed. Thus, in recent experiments, we compared ROSC rates using uncuffed versus cuffed ETTs. When using uncuffed ETTs, 7/19 piglets achieved ROSC, and when using cuffed ETTs, 5/5 piglets achieved ROSC (p = 0.012) (unpublished results). This finding supports the importance of a leak-free airway in this model.
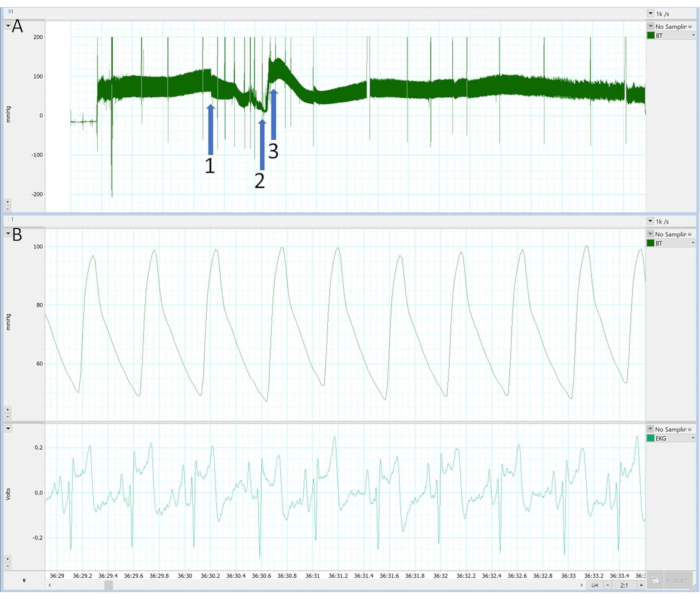
Figure 5: Continuous data sampling using the data acquisition and analysis software. An example of how continuous data sampling looks in the data acquisition and analysis software. (A) BP for the whole experiment. (B) Beat-to-beat complexes of BP and ECG. Different parts of the experiment are marked in panel (A): 1) start of asphyxia, 2) cardiac arrest and CPR, 3) ROSC. Please click here to view a larger version of this figure.
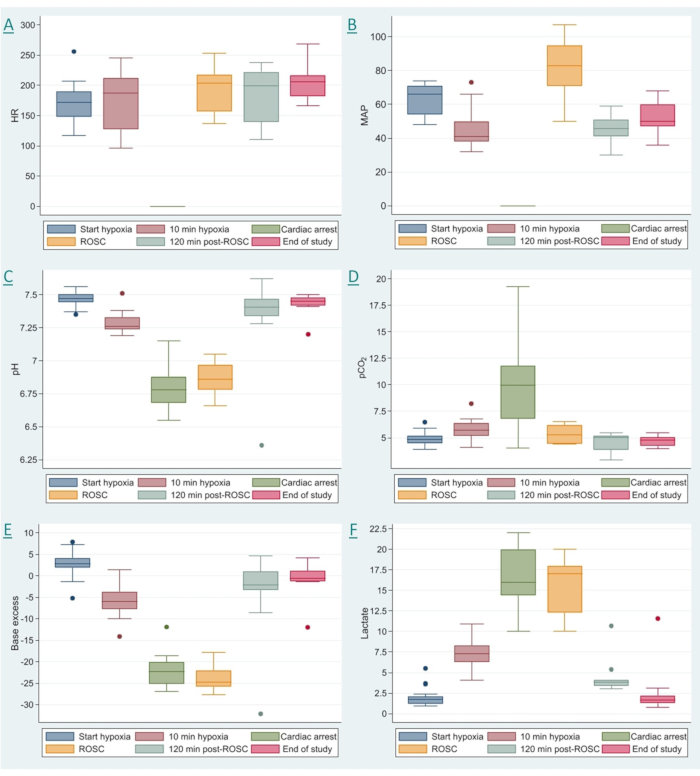
Figure 6: Changes in cardiovascular and metabolic variables throughout the experiment. A demonstration of how different variables change throughout the experiment. The six time points that are shown are as follows: just before the start of hypoxia (baseline), 10 min of hypoxia, cardiac arrest, ROSC, 120 min post ROSC, and the end of study (570 min post ROSC). (A) Heart rate (HR), (B) mean arterial pressure (MAP), (C) pH, (D) partial pressure of CO2 (pCO2), (E) base excess, and (F) lactate. Please click here to view a larger version of this figure.
