There are several findings that can be seen on the POCUS of the optic nerve sheath and several pitfalls that can occur in the measurements. As can be seen in Figure 5, the nerve typically heads back from the eye at an angle when the eye is in a neutral position. In patients undergoing elective ultrasound of the eye for optic neuritis, for example, the patient is typically asked to move the eye and straighten the nerve to facilitate the measurement of the diameter along the axis of the nerve. Patients with concern for TBI will rarely be able to follow commands, so the transverse diameter of the nerve sheath will need to be measured at an angle.
Another potential pitfall that can occur is a measurement of the optic nerve instead of the sheath. If appropriate settings are not used, or a low-resolution probe is used, such as those driven on a USB cable, it can be difficult to see the sheath, as is demonstrated in Figure 6. In this figure, two images are shown of the same patient, one demonstrating the nerve sheath and another, which was performed with a low-resolution probe, in which only the nerve is visible. It is important that the nerve sheath can be seen and measured for accuracy. The optic nerve itself does not change substantially in size with elevated ICP, so measuring the nerve instead of its sheath may give a false low measurement.
There are also several artifacts that can interfere with measuring the ONSD. A blooming artifact can confound the measurements. This artifact is hypothesized to be an acoustic shadow caused by the lamina cribrosa, which can be larger than the ONSD10. An example can be seen in Figure 7, where two images from the same patient are seen, one showing the optic nerve sheath and one showing a blooming artifact that is much larger in size. It is important that the head of the nerve be visualized as a rounded-off hypoechoic structure as it inserts into the posterior eye. The blooming artifact will extend from the optic disk and will not have a rounded-off head. Some authors11 recommend the use of color Doppler to clarify the course of the nerve and differentiate it from the blooming artifact. However, we do not think this is necessary for providers experienced in B-mode interpretation.
Normal findings vary, but in normal patients, the mean size of ONSD is 4.1 mm, and the ONSD cut-off value of 5.3 mm strongly predicts increased ICP (sensitivity: 94.7%; specificity: 84.3%)7. The average ONSD in patients with increased ICP is over 6 mm.
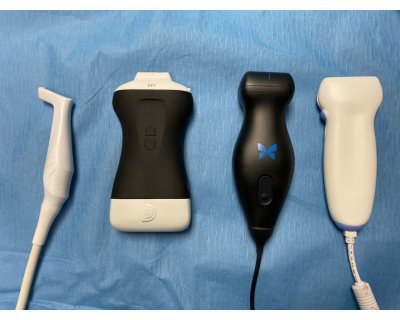
Figure 1: A series of representative ultrasound probes that can be used for ocular exams. From left to right: a 5-14 MHz probe with a 37 mm footprint (commonly referred to as a hockey stick probe) that can easily obtain transverse and sagittal views; a battery-powered handheld probe; an inexpensive USB probe with a 55 mm footprint that can acquire transverse images consistently and sagittal images on some patients; and a linear probe that cannot obtain sagittal views on most patients. Please click here to view a larger version of this figure.

Figure 2: A transparent adhesive dressing is used to keep the eyelid closed during scanning to protect the cornea. Please click here to view a larger version of this figure.
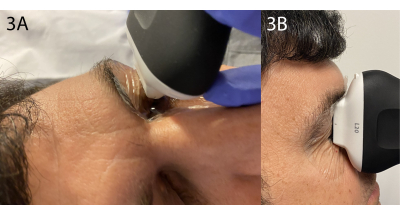
Figure 3: Transverse and sagittal views. (A) The transverse view is performed from the anteriormost aspect of the eye. The probe may need to be oriented slightly toward the midline to bring the nerve into the plane. (B) The sagittal view is performed in a similar fashion from the anteriormost aspect of the eye. Please click here to view a larger version of this figure.
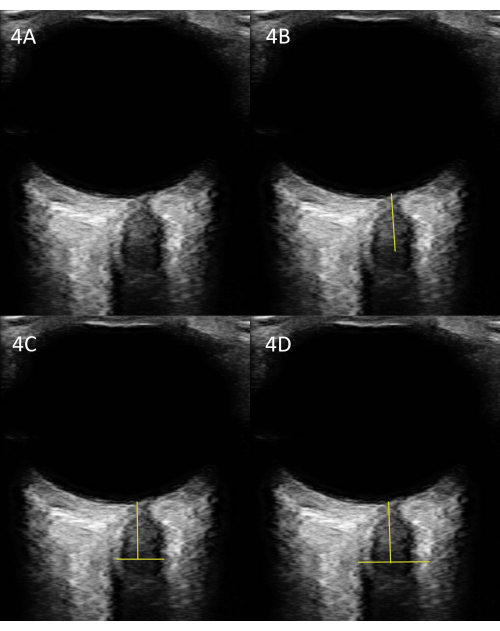
Figure 4: Measurement of the ONSD. (A) An unlabeled US image. (B) The same image with the appropriate place to measure the ONSD 3 mm posterior to the optic disk. (C) Transverse measurement of the optic nerve, not the sheath. (D) Measurement of the optic nerve sheath; this is the most relevant measure. Please click here to view a larger version of this figure.
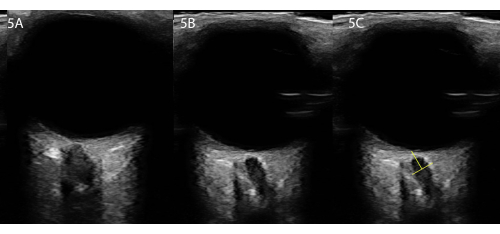
Figure 5: Imaging in patients with cooperative eye movements versus those who cannot cooperate. (A) If the patient is cooperative, have them move the eye so that the nerve is headed straight back, as in this example. (B) However, for severe TBI, the patient will not be able to cooperate, and the nerve will head back at an angle. (C) We recommend measuring along the axis of the nerve if it does not head straight back. Please click here to view a larger version of this figure.
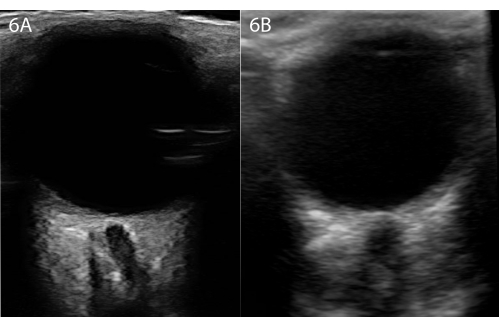
Figure 6: Two ultrasounds from the same patient at the same point in time. (A) The optic nerve sheath is visible. (B) US performed with an inexpensive USB-powered ultrasound; the nerve is visible, but not the sheath, even though this is the same patient. Please click here to view a larger version of this figure.
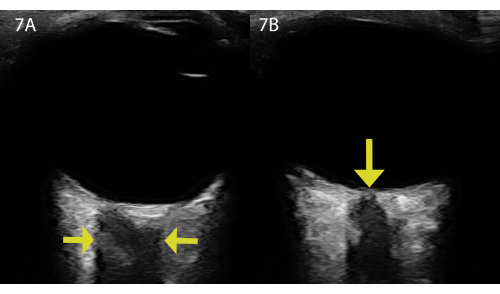
Figure 7: Two ultrasounds from the same patient and the same eye demonstrating a blooming artifact. (A) Demonstration of a blooming artifact from structures on the posterior eye. Note that there is no rounded nerve head, no sheath, and the shadow appears very rectangular. The arrows point to the sides of the blooming artifact. (B) The same patient with the optic nerve and sheath visible. Note that the rounded head of the nerve is demonstrated by the yellow arrow, and the sheath is visible. Please click here to view a larger version of this figure.
