Although the chronic effects of strength training on insulin sensitivity have been repeatedly shown1,2,3, even an acute session of strength exercise can improve insulin action for up to 48 h4. This effect has been demonstrated in healthy5,6,7,8, obese 9, older10, insulin-resistant individuals4, and type 2 diabetes mellitus patients11. Others have not reported positive effects12,13,14,15,16,17, and it is unclear why these differences occur.
In a recent narrative review18, it was suggested that strength exercise volume (the number of sets per exercise) is essential to improve insulin sensitivity. For instance, a recent systematic review and meta-analysis demonstrated that sessions composed of 21 sets or more led to a greater improvement in insulin action compared to sessions with fewer than 21 sets19. However, only limited evidence from literature directly supports this notion. For example, higher strength exercise volume (30 sets) improved glucose metabolism more than lower volume (10 sets)20. But it is worth noting that this study implemented circuit-style strength exercises, which limits the comparison to traditional strength exercises. In another study, better insulin sensitivity was observed after a 32-set strength exercise protocol compared to an 8-set protocol21. However, the degree of effort after sets was not reported, and it was presumably greater after the high-volume protocol. This is important because the degree of effort (or proximity to concentric muscular failure, characterized as the inability to continue the set due to failure in the concentric movement of a given repetition) has also been considered an important variable to improve insulin and glucose metabolism18. Thus, the limited available studies on the topic, along with their methodological limitations, preclude further inferences regarding the effects of strength exercise volume on insulin sensitivity.
Another interesting point when discussing strength exercise volume is that it is inherently connected to time commitment. A lower exercise volume, by design, means less time spent in the gym. Among the reasons for not adhering to an exercise program, lack of time is at the top of the list22. Thus, a low-volume strength exercise session that effectively improves insulin sensitivity means less time commitment23 and might result in higher long-term adherence. Furthermore, subjective feelings, such as self-efficacy (self-perception of the ability to accomplish something) and the sensations of pleasure and fun (enjoyment), are also related to exercise adherence24,25,26. It is reasonable to speculate that people might feel more confident and enjoy their exercise experience more when they perform a low-volume strength exercise session that translates into health improvement.
To address the gaps in the literature summarized above, we describe a protocol for a randomized, controlled, crossover, clinical trial with the primary aim of assessing the effects of strength exercise volume on insulin sensitivity in obese individuals. As a secondary aim, we assess the effects of strength exercise volume on subjective feelings (self-efficacy, affection, and enjoyment).
The protocol here describes a randomized, controlled, 3-way, crossover, clinical trial. The chronological sequence of the protocol includes: a pre-participation assessment of health history and anthropometric measures (body mass, height, waist circumference, and body composition); an appointment with the team's certified nutritionist; a familiarization period with the strength exercises and subjective feelings questionnaires; strength assessment in each exercise; random allocation of the order of the sessions; performance of the 3 sessions (separated by 7-28 days), that is immediately followed by answering the subjective feelings questionnaires; an oral glucose tolerance test (OGTT) the next morning; and data analysis. Figure 1 delineates the protocol design.
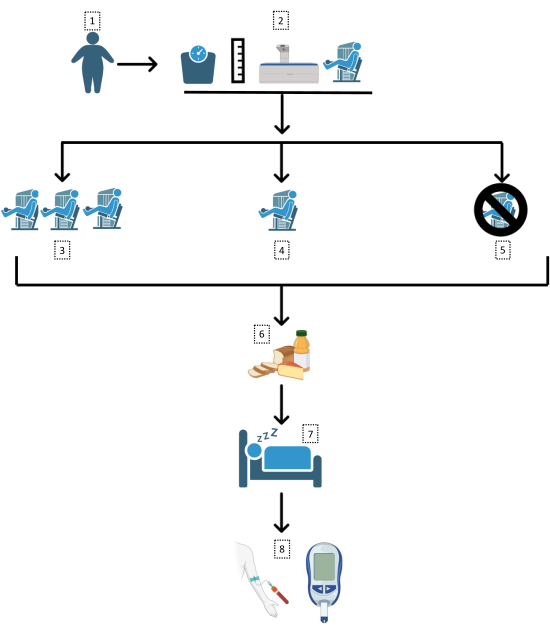
Figure 1: Study design. A flowchart of the trial methodology followed here. 1: Obese (body mass index [BMI] >30 kg/m2; waist circumference >102/88 cm) subjects; 2: Anthropometric assessments and familiarization; random assignment to 3: high-volume strength exercise session (21 sets), 4: low-volume strength exercise session (7 sets), or 5: control day; 6: standard meal following sessions; 7: sleep and overnight fast; 8: oral glucose tolerance test. Please click here to view a larger version of this figure.
Figure 2 shows representative (from a pilot study) responses for glucose (Figure 2A) and insulin (Figure 2B) during the OGTT. Usually, peaks for glucose and insulin values are observed at 30 min measurement, which is followed by a constant decrease until 120 min measurement. The lower the glucose peak, the better the result, which is indicative of inhibition of hepatic glucose production. The faster the decrease in glucose after the peak, the better the result, which is indicative of faster glucose disposal (usually associated with skeletal muscle glucose uptake). For insulin, lower values indicate that less insulin is needed to be released by pancreatic beta cells for glycemia control. However, this interpretation is only valid for individuals with functional beta cells, as individuals with dysfunctional (or dead) beta cells will have lower insulin response during the OGTT, but higher glycemic response.
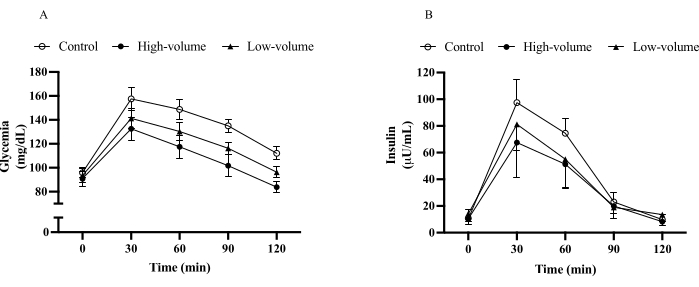
Figure 2: Oral glucose tolerance test. Glycemia (A) and insulin (B) responses to oral glucose tolerance test after no exercise (control), 21 sets strength exercises (high-volume), and 7 sets strength exercises (low-volume) protocols in obese adults. Data shown as mean (bars) and standard deviation (error bars). Please click here to view a larger version of this figure.
Figure 3 shows insulin sensitivity indexes derived from the OGTT. The most common are glucose (Figure 3A) and insulin (Figure 3B) AUC. Notice that lower AUC indicates a better result. In other words, individuals that show lower glycemia and insulin concentration after a standard glucose challenge likely have better insulin sensitivity. Other insulin sensitivity indexes can be calculated from the results of the OGTT (Figure 3C-I). As they use different parameters from the OGTT to estimate insulin sensitivity, the results vary among indexes. However, the pattern is similar for most indexes as low- and high-volume strength exercises improve insulin sensitivity, but superior outcomes are observed following the latter condition.
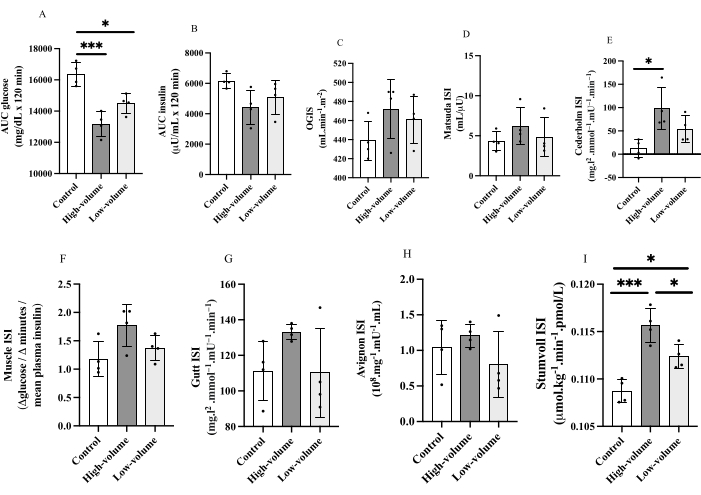
Figure 3. Insulin sensitivity indexes. Oral glucose tolerance test-derived insulin sensitivity (IS) indexes (ISI) responses after no exercise (control), 21 sets strength exercises (high-volume), and 7 sets strength exercises (low-volume) protocols in obese adults. Glucose (A) and insulin (B) area under the curve (AUC), oral glucose (OG) IS (C), Matsuda ISI (D), Cederholm ISI (E), Muscle ISI (F), Gutt ISI (G), Avignon ISI (H), and Stumvoll ISI (I). *p<0.05; ***p<0.001 for Tukey post-hoc test. Data are shown as individual values (plots), mean (bars) and standard deviation (error bars). Please click here to view a larger version of this figure.
