The key instruments used to perform the dMCAO are the microsurgical instruments set, the isoflurane vaporizer, and the monopolar microsurgical electrocoagulation generator shown in Figure 1. The experimental procedure of this study is illustrated in Figure 2. In brief, a small bone window craniotomy was employed to expose the distal MCA, which was subsequently coagulated to induce permanent focal cerebral ischemia in C57BL/6 mice. Furthermore, the ischemic insults and stroke outcomes were assessed through TTC staining, histological examinations, and behavioral evaluations at 3 days post dMCAO. During the surgical procedure, only 1 mouse died from surgical bleeding. Furthermore, all the remaining mice survived during the 3-day observation period after surgery.
Macroscopic observation revealed that the dMCAO generated visible hyperemia and edema in the cortex (Figure 3A, bottom). No discernible macroscopic alterations were observed in the sham-operated group (Figure 3A, top). Additionally, dMCAO-induced cortical infarction was also verified using TTC staining (Figure 3B). The infarct volume was 16.6% ± 0.8% 3 days after the surgery in the dMCAO group, demonstrating the stability and repeatability of this cerebral ischemia model (Figure 3C).
Several behavioral tests were conducted to evaluate the neurological deficits on 3rd day post dMCAO. As shown in Figure 4A, the fore limb grip strength exhibited a significant reduction in the dMCAO group compared to the sham-operated group (70.8 g ± 4.2 g vs. 114.0 g ± 6.2 g, P < 0.001). The dMCAO group mice exhibited prolonged latencies in both turning around and descending to the ground during the pole test, as compared to the sham-operated group (15.8 s ± 1.7 s vs. 8.7 s ± 1.3 s, P < 0.01, 45.1 s ± 3.3 s vs. 29.2 s ± 2.1 s, P < 0.001) (Figure 4B,C). For the adhesive removal test, a significant increase in the removal time was observed in the dMCAO group compared to the sham operation group (20.5 s ± 2.5 s vs. 7.8 s ± 1.1 s, P < 0.001) (Figure 4D). The statistical analysis of the cylinder test data demonstrated a significant reduction in contralateral forepaw usage rates within the dMCAO group compared to the sham operation group (35.2% ± 2.6% vs. 48.7% ± 2.2%, P < 0.001) (Figure 4E).
Black squares in Figure 5A illustrate the analysis region for immunofluorescent staining. The H&E staining results revealed the disordered arrangement of neuron cells in the peri-infarct area of the dMCAO group, characterized by prominent pyknosis, vacuolization, and nuclear hyperstaining (Figure 5B, bottom). However, the sham-operation group did not exhibit any discernible alterations in neuronal morphology (Figure 5B, top). Figure 5C illustrates that dMCAO resulted in a significant reduction in the density of NeuN-positive cells within the peri-infarct area (319.6 ± 19.0 vs. 765.0 ± 26.0, P < 0.001). Figure 5D,E illustrates that the densities of microglia (665.8 ± 30.6 vs. 207.4 ± 16.2, P < 0.001) and astrocytes (305.2 ± 17.2 vs. 17.2 ± 2.1, P<0.001) increased greatly in dMCAO group compared with the sham-operation group. These findings offer compelling evidence supporting the presence of neuronal loss and the excessive activation of microglia and astrocytes on the 3rd day post-dMCAO.

Figure 1: Key instruments used to establish the dMCAO model. (A) Essential surgical instruments. The Roman numerals I-VII refer to electric coagulation forceps, curved micro forceps, micro scissors, straightmicro forceps, retractors, needle holders, and surgical scissors. (B) Isoflurane vaporizer. (C) Electro-surgical generator. Please click here to view a larger version of this figure.
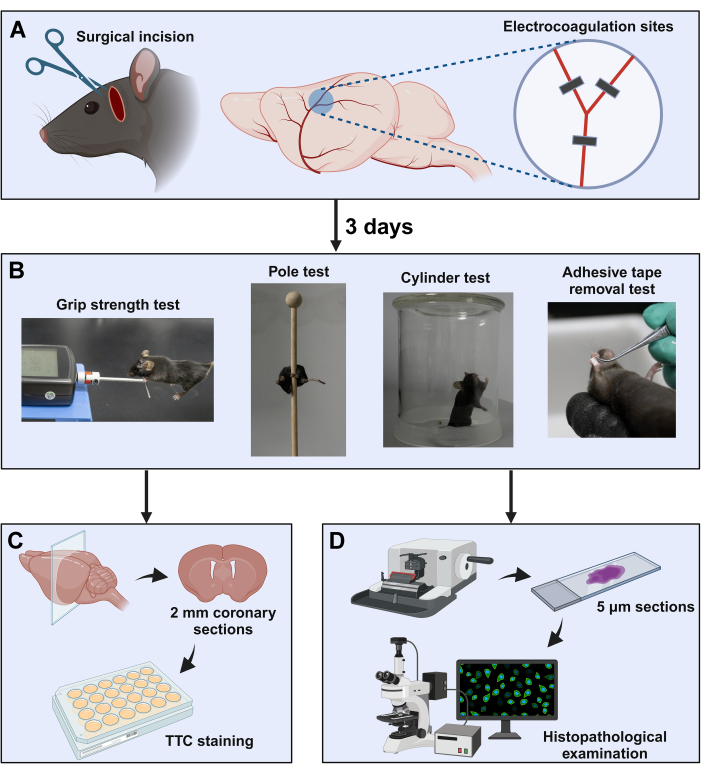
Figure 2: Schematic diagram of the experimental procedure. (A) The surgical window is located between the orbit and the ear canal. The distal MCA was exposed by subtemporal craniotomy, followed by coagulation at three sites near the bifurcation (indicated with black squares). (B) Neurological behavior evaluation paradigms were used in this study. After completion of the neurological behavior tests, the brain samples were collected for (C) TTC staining and (D) histopathology examinations. Please click here to view a larger version of this figure.
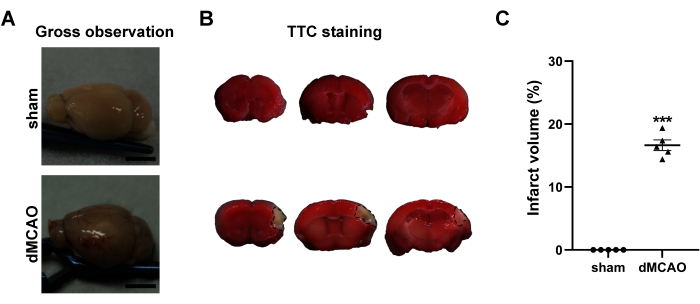
Figure 3: Macroscopic evaluation of the brains at 3rd day post dMCAO. (A) Gross observation of the brains from the sham operation and dMCAO groups. (B) Representative TTC-stained brain coronary sections of sham operation group (top) and dMCAO group (bottom). The black line demarcates the non-infarcted (unstained) cortex of the ipsilateral brain. (C) Quantification of the infarct volume. Scale bar = 5 mm. Data are presented as mean ± SEM. N = 5, ***P < 0.001 compared with the sham group, paired t-test. Please click here to view a larger version of this figure.
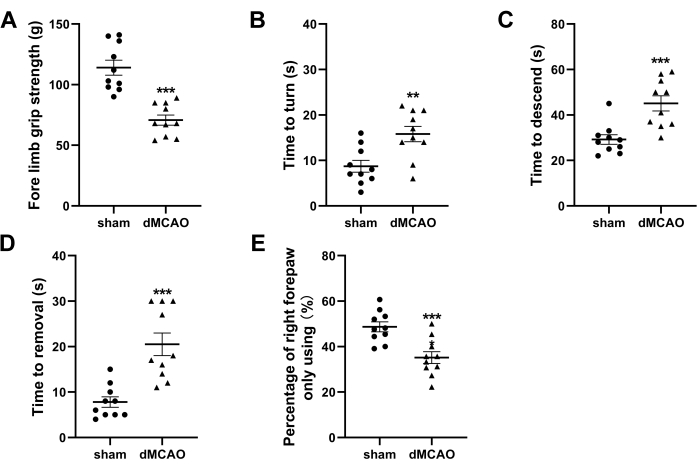
Figure 4: Neurological behavior tests at 3rd day post-dMCAO. (A) Quantification ofthefore limb grip strength. (B,C) Quantification of the time latencies to turn around and descend to the ground in the pole test. (D) Quantification of time required to remove the adhesive tape in the adhesive removal test. (E) Quantification of cylinder test presented as the usage ratio of the right forepaw. Data are presented as mean ± SEM, N = 10, **P < 0.01, ***P < 0.001 compared with the sham group, paired t-test. Please click here to view a larger version of this figure.
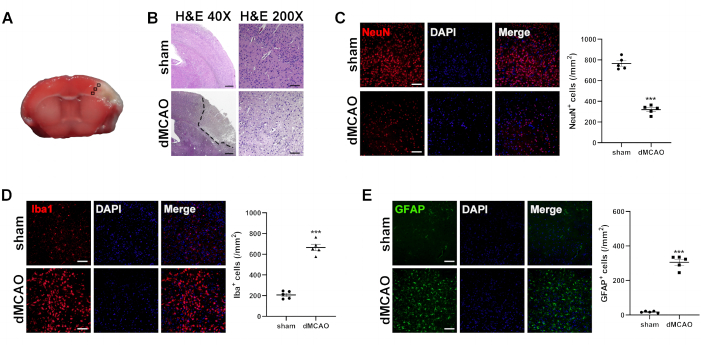
Figure 5: Histological analysis of brains at 3rd day post dMCAO. (A) Immunofluorescence measurement from the cortex of the selected three fields in the ischemic penumbra. (B) Representative images of H&E-stained brain sections from the sham operation and dMCAO groups. Dotted lines surround unstained parts, indicating an infarct lesion. (H&E 40x, Scale bar = 200 µm; H&E 200x, Scale bar = 50 µm). Representative images of immunofluorescence staining and quantitative analysis for (C) NeuN (a marker for neuron), (D) Iba-1 (a marker for microglia), and (E) GFAP(a marker for astrocyte). Scale bar = 50 µm. Data are presented as mean ± SEM, N = 5, ***P < 0.001 compared with the sham group, paired t-test. Please click here to view a larger version of this figure.
