We performed a preliminary descriptive analysis of the first randomized subject without unblinding the study. For this reason, which arms this subject was allocated to is unknown. The first subject is a 69-year-old woman, non-Hispanic, Caucasian, with a college degree, who did not report any adverse event during or after the stimulation session. The clinical data are displayed in Table 2.
Besides, a topographic distribution of scalp plots was created in resting-state EEG for theta, alpha, and beta bands in three time periods: baseline, during, and post-procedure (Figure 7). An asymmetric alpha pattern was noticed in the frontal region.

Figure 1: Main taVNS Device, with bilateral electrodes. Please click here to view a larger version of this figure.

Figure 2: Earset of the taVNS device. Please click here to view a larger version of this figure.

Figure 3: Conductive Ear tip of the electrodes of the taVNS device. Please click here to view a larger version of this figure.
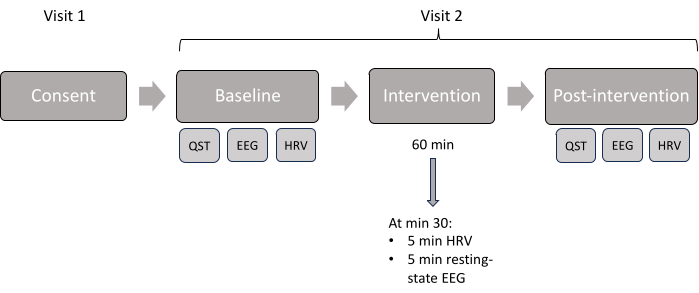
Figure 4: Study visit scheme. Displayed chronologic order of the assessments done in each visit. Please click here to view a larger version of this figure.
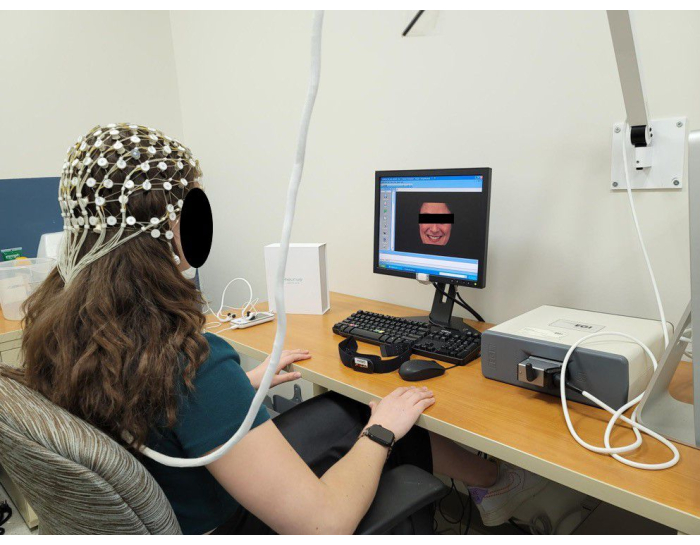
Figure 5: Representation of a subject during an EEG session using a 64-channel EGI system. Please click here to view a larger version of this figure.

Figure 6: Representation of a subject during the EEG session plus taVNS stimulation. Please click here to view a larger version of this figure.
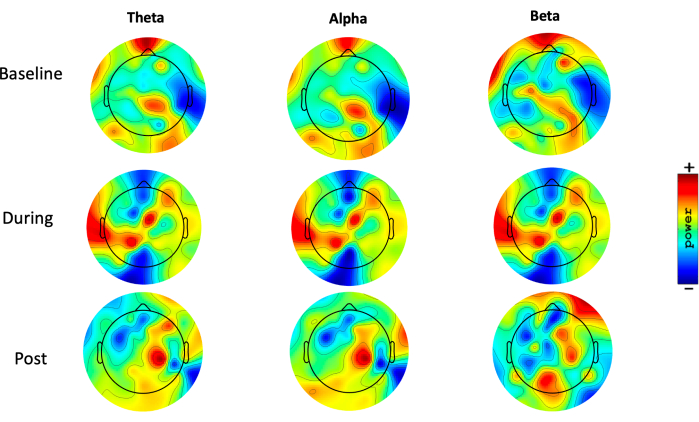
Figure 7: Topographic distribution. Topoplots, showing the topographic distribution of the theta (1-3.9 Hz), alpha (8-12.9 Hz), and beta (13-29.9 Hz) power (range 35 to 44 dB) (10 x log10 P), during resting-state EEG, in three different moments: pre-intervention (baseline), during intervention, and after intervention (post). Blue areas represent low activity, and red areas represent high activity. Please click here to view a larger version of this figure.
| Consent and screening | Baseline | Intervention | Post intervention | |
| Visit 1 (online) | Visit 2 | Visit 2 | Visit 2 | |
| Demographics | X | |||
| Medical History | X | |||
| Consent form | X | |||
| Beck depression inventory | X | |||
| EHI/SF | X | |||
| Pregnancy test | X | |||
| BMIS | X | X | ||
| VAS-F | X | X | X | |
| EEG | X | X | X | |
| HRV | X | X | X | |
| QST | X | X | ||
| Success of blinding questionnaire | X | |||
| Approximate visit time | 60 min | 60 min | 60 min | 30 min |
Table 1: Assessments scheme. "X" indicates that the procedures were done in each of the visits.
| Variable | Demographic data | Baseline | During intervention | After intervention |
| Age (years) | 69 | |||
| Gender | Female | |||
| Ethnicity | Non-Hispanic | |||
| Race | Caucasian | |||
| Education level | College degree | |||
| Pain 60 | 47 | . | 44 | |
| TS | 3 | . | 1 | |
| CPM | 4 | . | 5 | |
| Mood | -6 | . | 9 | |
| Fatigue | 5.7 | 6.6 | 6.76 | |
| HRV – HF | 0.046 | 0.066 | 0.584 | |
| HRV – LF | 0.073 | 0.043 | 0.037 |
Table 2: The clinical data representative of one subject.
