Acetylcholine dose-response protocol
Figure 1A depicts a schematic detailing the ACh dose-response protocol. Figure 1B illustrates representative tracings of the RBC flux values (perfusion units, PU; 30 s averages) from the standardized ACh dose-response protocol for one subject over time. Figure 1C illustrates a raw data file of an ACh dose-response protocol. Additional baseline measurements were maintained in the raw data file, but only ~10 min of baseline were utilized for the data analysis.
Following hyperemia resolution and a stable RBC flux for 5 min, the 10 min baseline data collection may begin. The baseline is depicted as a relatively stable horizontal RBC flux line, where any cause for deviations (e.g., movement artifacts, probe adjustments) should be logged as data acquisition software comments for analysis purposes. The dose-response protocol follows the baseline period, and the syringes must be changed with each dose, from 10−10 M to 10−1 M ACh. Before starting the 5-10 min perfusion of each dose, one must ensure that the pharmacological agent has fully perfused through the length of the fiber. In the data acquisition software, there will be an initial rise in the RBC flux due to the perfusion, but this is not included in the analyses, as the 5 min data collection for that concentration has not begun. Once the perfusion for each dose has begun, there will be a continual increase in the RBC flux to a peak, followed by a steady decline. This curvilinear response to pharmacological agents will be replicated throughout the protocol, but the RBC flux will be relatively greater with increasing concentrations of ACh. With lower concentrations of ACh, the curvilinear response may not be as prominent. Examples of non-optimal RBC flux include the following: 1) a non-curvilinear response, where the RBC flux does not increase and remains plateaued, or 2) increasing ACh concentrations having a minimal impact on the RBC flux, where the RBC flux does not relatively increase with each concentration of ACh. This is dependent on the research question and the clinical cohort being tested.
Following the final concentration of ACh, lactated Ringer's is perfused, and the local heaters are increased to 43 °C. During this phase, a plateau must be obtained before sodium nitroprusside is perfused. This may take up to ~45 min, depending on the previous agents perfused. This phase is not included in the analyses. Once the plateau has been obtained for 5 min, sodium nitroprusside is perfused to produce maximal local vasodilation. This maximal local vasodilation is depicted as a rise in the RBC flux, where a plateau is obtained after ~20 min of perfusion, or by the RBC flux reaching a peak and declining immediately after. Once a plateau or a decline in the RBC flux has been obtained for sodium nitroprusside, the protocol is complete. A common example of non-optimal RBC flux is the highest value of RBC flux being obtained at a different phase of the protocol (e.g., during the dose-response protocol) rather than during the maximal local vasodilation.
Acetylcholine dose-response protocol: Nitric Oxide synthase inhibition
To quantify the contribution of NO to cutaneous blood flow in response to ACh, NG-nitro-l-arginine methyl ester (L-NAME), a NO synthase inhibitor, is perfused in combination with ACh through an additional fiber. Figure 2A depicts a schematic detailing the ACh dose-response protocol with L-NAME. Figure 2B illustrates representative tracings of the RBC flux (30 s averages) from the standardized ACh dose-response protocol for one subject over time with L-NAME. Figure 2C illustrates a raw data file of an ACh dose-response protocol with L-NAME. Additional baseline measurements were maintained in the raw data file, but only ~10 min of baseline were utilized for the data analysis.
Following hyperemia resolution, a stable RBC flux for 5 min, and adequate time to fully block the enzymatic pathway of interest (e.g., NO synthase) and/or deliver adequate concentrations of co-factors, the 10 min of baseline data collection may begin (depicted as a relatively stable horizontal line). The dose-response protocol follows baseline, and the syringes must be changed with each dose starting from 1010 M to 101 M ACh with the NO synthase inhibitor (e.g., 15 mM L-NAME). In the presence of a NO synthase inhibitor, the curvilinear response is not well replicated until higher concentrations of ACh. A relatively lower RBC flux, in comparison to a site without NO synthase inhibition, will be observed. A common example of non-optimal RBC flux is the NO synthase inhibition, as compared to the conditions without NO synthase inhibition, resulting in a higher RBC flux. This indicates that the protocol has failed.
Following perfusion of the final concentration of ACh, lactated Ringer's is perfused, and the local heaters are increased to 43 °C. During this phase, a plateau should be obtained before sodium nitroprusside is perfused. This phase is not included in the analyses. Once the plateau has been obtained for 5 min, sodium nitroprusside is perfused, producing maximal local vasodilation. During maximal local vasodilation, there will be an exponential rise in the RBC flux due to the previous NO synthase inhibition. A plateau will be obtained after ~20 min of perfusion, or the RBC flux will reach its absolute peak and decline immediately after. Once a plateau or a decline in the RBC flux has been obtained for sodium nitroprusside, the protocol is complete. A common example of non-optimal RBC flux is obtaining the highest RBC flux value at a different phase of the protocol (e.g., during the dose-response protocol) rather than during the maximal local vasodilation.
Local heating protocol
Figure 3A depicts a schematic detailing the local heating protocol. Figure 3B illustrates representative tracings of the RBC flux (30 s averages) for the standardized local heating protocol for one subject over time. Figure 3C illustrates a raw data file of a local heating protocol. Following hyperemia resolution and a stable RBC flux for 5 min, the 10 min of baseline data collection may begin (depicted as a relatively stable horizontal line). The local heaters are set to either 39 °C or 42 °C, and an initial peak and nadir response will occur in the RBC flux. To quantify the contribution of NO to the cutaneous blood flow in response to a local heat stimulus, L-NAME is perfused after a stable plateau in the RBC flux has been achieved. There will be a rapid decline in the RBC flux until it reaches a new plateau in response to L-NAME. After 5 min of stable RBC flux values, lactated Ringer's is perfused, and the local heaters are increased to 43 °C. The heating will produce an additional peak and nadir response in the RBC flux. During this phase, one must ensure that a plateau has been obtained before sodium nitroprusside is perfused. This phase is not included in the analyses. To induce local maximal vasodilation, sodium nitroprusside is perfused, and a rapid increase in the RBC flux will occur. Once a plateau or a decline in the RBC flux has been observed in response to sodium nitroprusside, the protocol is complete.
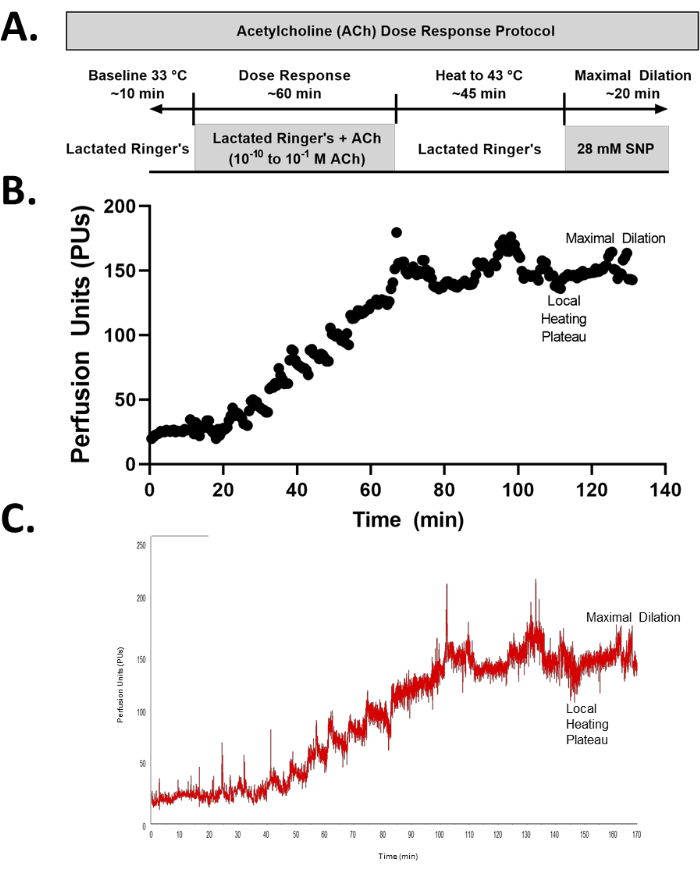
Figure 1: Acetylcholine (ACh) dose-response protocol. (A) Schematic of an ACh dose-response protocol. (B) Representative tracing (30 s averages) of an ACh dose-response protocol. (C) Raw data of an ACh dose-response protocol. Additional baseline measurements are maintained in the raw data file to demonstrate the fluctuations prior to stabilization, but only ~10 min of stable resting data were utilized for the data analysis. Please click here to view a larger version of this figure.
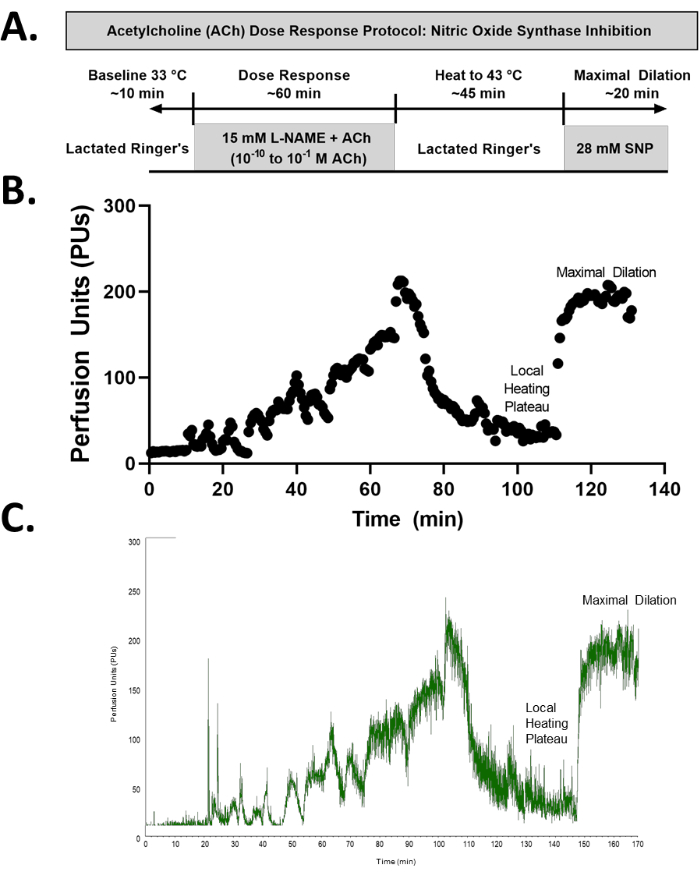
Figure 2: ACh dose-response protocol with Nitric Oxide (NO) synthase inhibition. (A) Schematic of an ACh dose-response protocol with NO synthase inhibition. (B) Representative tracing of an ACh dose-response protocol with NO synthase inhibition. (C) Raw data of an ACh dose-response protocol with NO synthase inhibition. Additional baseline measurements are maintained in the raw data file to demonstrate the fluctuations prior to stabilization, but only ~10 min of stable resting data were utilized for the data analysis. Please click here to view a larger version of this figure.
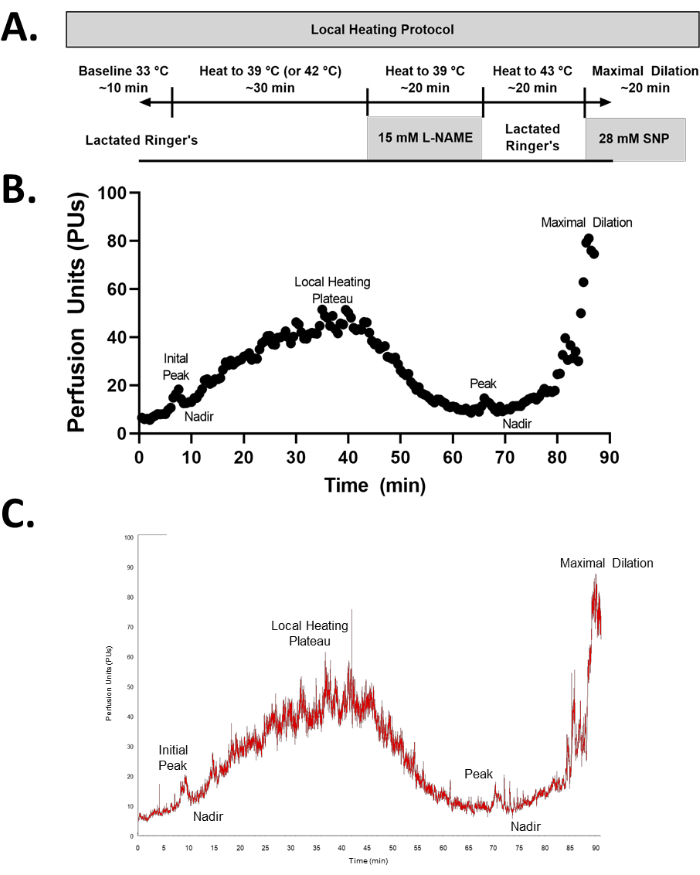
Figure 3: Local heating protocol. (A) Schematic of a local heating protocol. (B) Representative tracing of a local heating protocol. (C) Raw data of a local heating protocol. Please click here to view a larger version of this figure.
