The extent of myocardial infarction can be assessed by Evans blue/2,3,5-triphenyltetrazolium chloride (TTC) double staining. TTC is a redox indicator, which is converted to deep-red 1,3,5-triphenylformazan in living tissues due to the activity of various dehydrogenases in the presence of NADH8. Figure 1 shows a representative section of the heart at 24 hr after ligation of the left anterior descending coronary artery. Blue-stained areas indicate non-ischemic/normal regions. The myocardial area at risk is defined as the myocardial tissue within the perfusion bed distally from the ligation of the left anterior descending coronary artery. Deep-red-stained areas indicate ischemic but viable regions (non-infarcted area at risk) regions whereas negatively stained areas (pale red) indicate infarcted regions. In this model, the non-infarcted area at risk is negligible and not visible in this image, which reflects the permanent character of the ligation of the left anterior descending coronary artery. The infarcted area is typically between 50 – 60% of the total left ventricular wall area9,10. Two components in the evolution of the infarct zone should be discerned: 1) the three-dimensional geometry of the infarct may alter as a consequence of infarct expansion leading to a thinner but more extended myocardial infarction, and 2) the total volume of the infarct may decrease, which reflects the healing process with wound contraction and scar formation.
Infarct expansion can be quantified by evaluating the time-course of infarct length and infarct thickness10. A representative Sirius Red stained cross-section of a heart at day 28 after permanent ligation of the left anterior descending coronary artery is shown in Figure 2. The image shows an infarct that has been substantially stretched. In a cross-section, this expansion corresponds to an increase of the absolute infarct length and a decrease of infarct thickness.
Besides considerations on the three-dimensional geometry and the volume of the infarct, another caveat with regard to interpretation of infarct parameters should be considered. Since the viable myocardial tissue will also undergo hypertrophy, it is clear that the ratio of infarct area versus total left ventricular wall area will decrease as a function of time. Assessment of longitudinal changes of the infarct zone requires therefore a clear insight in the difference between absolute parameters and relative parameters.
An arterial and ventricular pressure register is shown in Figure 3. After stabilization of the catheter, heart rate, maximal systolic left ventricular pressure, minimal diastolic left ventricular pressure, the peak rate of isovolumetric left ventricular contraction (dP/dtmax), the end-diastolic left ventricular pressure, and the peak rate of isovolumetric left ventricular relaxation (dP/dtmin) are determined. The time constant of isovolumetric left ventricular pressure fall (tau) is quantified using the method of Weiss et al.7.

Figure 1. Assessment of area at risk and infarct size 1 day after myocardial infarction. The images from left to right go from the cardiac apex to the base of the heart. 24 hr after permanent ligation of the left anterior descending coronary artery, 2 ml of Evans blue dye was injected as a bolus into the aorta to quantify the volume of the perfused myocardium. Hearts were subsequently arrested in diastole by injection of CdCl (100 µl; 0.1 N), were flushed with physiological saline to wash out excess blue dye, and were embedded in 5% low gelling temperature agarose. Afterwards, 500 µm thick cross-sections were made using a HM 650 V Vibration Microtome and slices were then incubated in a 1.5% 2,3,5-triphenyltetrazolium chloride containing isotonic phosphate buffer (pH 7.4) for 30 min at 37 °C. Images were made using a SteREO Lumar V.12 microscope. The negatively stained area of infarcted tissue, the red-stained non-infarcted area at risk, and the blue-stained non-ischemic healthy ventricular wall area were quantified using Image J software. Scale bar represents 0.5 mm. Please click here to view a larger version of this figure.
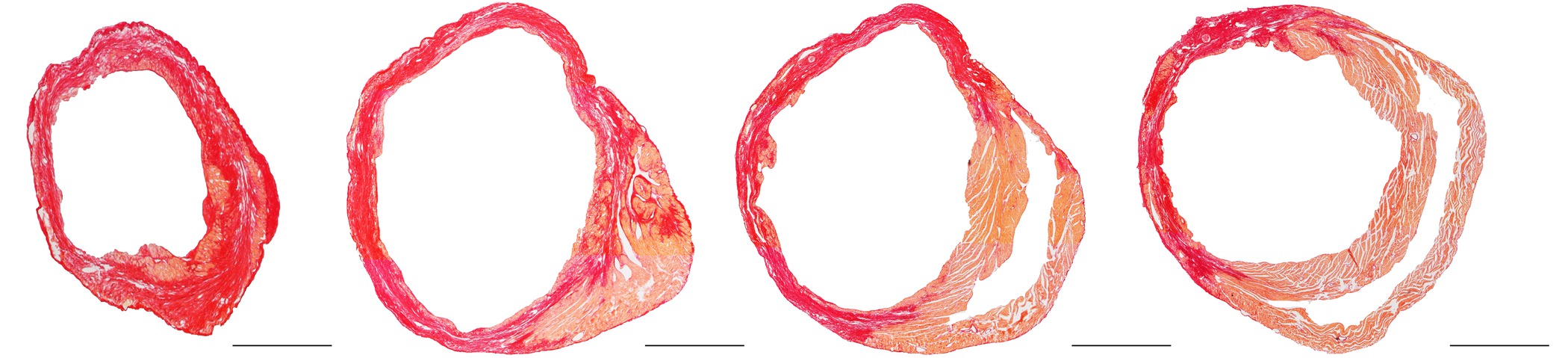
Figure 2. Representative Sirius Red stained cross-section of a heart at day 28 after ligation of the left anterior descending coronary artery. The images from left to right go from the cardiac apex to the base of the heart. The standard protocol of Junqueira et al.11 was applied for Sirius Red staining. This histochemical method stains fibrotic infarct tissue dark red and healthy tissue orange. Scale bar represents 1 mm. Please click here to view a larger version of this figure.
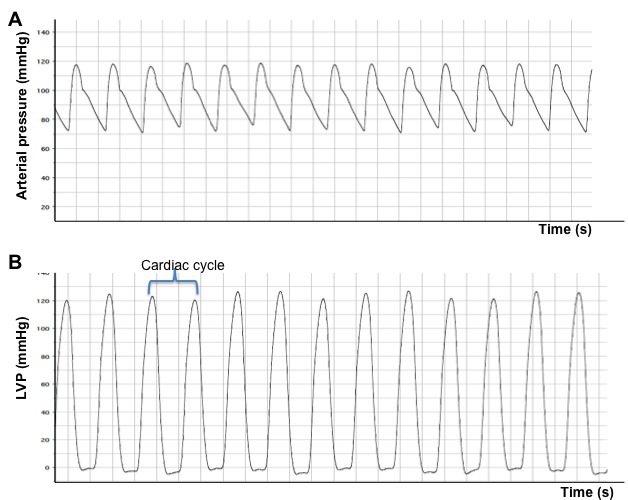
Figure 3. Arterial (A) and left ventricular (B) pressure registers obtained after catheterization of normal mice. The obvious difference between an arterial signal and a ventricular signal is that the latter signal drops to approximately 0 mm Hg during diastole. LVP: left ventricular pressure.
