All blood-drawing procedures should be done by licensed and certified professionals. Use of human subjects for research involves approval from the Institutional Review Board or other appropriate authority. Special precautions regarding informed consent and protecting participant identification need to be followed. All experiments listed in this protocol involve handling of human blood and/or blood products and appropriate personal protective equipment need to be worn at all times. The waste should be considered as biohazard and disposed of according to regulations.
1. Venipuncture
- Identify the patient/ participant and confirm with existing records. Explain the study in detail and get an informed consent.
- Have a tray set up for individual patient with tubes marked on a flat stable surface.
- Explain the procedure and make the patient seat comfortably with the arm supported. Inform the patient that he or she will feel a small pinch and should remain still throughout the procedure.
- Attach the needle to the adapter.
- Wash hands and wear gloves.
- Prepare the antecubital fossa for venipuncture by cleaning with 70% isopropyl alcohol in concentric circles from center outward. Allow the site to air-dry for 30 sec.
- Identify the appropriate vein by palpation.
- Apply the tourniquet 3-4 in above the puncture site making sure that it is not too tight (while still feeling the radial pulse).
- Perform venipuncture by inserting the bevel of the needle 15-30 degrees to the skin in one smooth motion. Push the blood collection tube through the needle and collect 9 ml of whole blood.
- Remove the tourniquet. Remove the tube from the needle.
- Withdraw the needle and apply the gauze square at the puncture site prior to needle removal. Dispose the needle in an appropriate biohazard container.
- Ask patient to maintain pressure at the puncture site.
- Label the tubes
- Check the puncture site to be sure bleeding has stopped.
- Apply adhesive bandage or tape over the gauze square, ask if the patient is feeling alright (no pain, swelling or light headedness)
- Thank the patient/participant prior to discharge.
2. L-PRF Preparation
- Immediately after venous blood collection in the red-topped dry glass tube, place it in the Centrifuge.
- Centrifuge at 400 x g for 12 min at RT after placing an appropriate counter balance.
- Remove the tube at the end of the cycle. Notice the three layers: platelet-poor plasma (PPP), platelet-rich fibrin (L-PRF) and RBC base (Figure 1).
- Aspirate the PPP using a pipette. Using tweezers gently pull the L-PRF out and place it in a sterile, perforated metal mesh.
- Using surgical scalpel, scrape the bulk of RBC layer carefully leaving the buffy coat intact.
- Gently compress the L-PRF clot (using the sterile metal plate, approximate weight 225 g) for 30 sec. Platelet poor plasma will be squeezed out.
- Remove the plate and gently lift the L-PRF membrane. The L-PRF membrane is ready for use in experiments12.
3. Uniaxial Tensile Testing
- Place L-PRF membranes (n=6) on a filter paper for ease of handling and punch into “dog bones” using custom-made metal dies (2.75 mm wide at their narrowest point with a gauge length of 7.5 mm).
- Measure the thickness of each sample at three spots and take the average.
- Carefully engage the L-PRF membrane in the center of the jaw grips of the uniaxial testing system.
- Carefully tear the filer paper support to expose the L-PRF membrane.
- Program the instrument so that the movable head is operating at a constant rate (10.0 mm/min) and start the experiment when the L-PRF is still wet.
- Record the elastic modulus, energy to break, and strain at break from the software accompanying the uniaxial testing system. These values are calculated automatically and no user defined input is required. Please see Figure 3.
4. Suture Retention Strength
- Place L-PRF membranes (n=3) on a filter paper for ease of handling and cut into rectangular samples measuring (10 mm x 25 mm) using a surgical scalpel.
- Measure the thickness of each sample (average of 3).
- Make a pinhole in the center of the sample using the stainless steel orthodontic ligature wire (220 µm in diameter).
- Pass the ligature wire through the pinhole to form a loop and fix it to the tensile testing machine. Place the edge of the L-PRF membrane to the lower jaw grip13.
- Program the instrument so that the movable head is operating at a constant rate (10 mm/min) and start the experiment.
- Record the elastic modulus, energy to break, and strain at break from the software accompanying the uniaxial testing system. These values are calculated automatically and no user defined input is required. Please see Figure 3.
5. Morphological Examination
- Prepare the L-PRF samples for SEM examination using a 10 mm dermal biopsy punch and place them in a 24-well plate.
- Wash the samples with PBS and fix with 2.5% glutaraldehyde (in PBS) for 20 min.
- Dehydrate the specimens by immersion in sequentially increasing concentrations of ethanol (50%, 70%, 80%, 90% and 100%) for 5 min each.
- Treat with 0.5 ml of 100% HMDS (Hexamethyldisilazane) for 5 min. Aerate O/N to remove excess HMDS14.
- Mount samples on stubs using a double-sided tape, sputter-coat platinum for 70 sec and examine in a scanning electron microscope operating at an acceleration voltage of 20 kV (or appropriate setting).
6. Genipin Crosslinking of L-PRF, Trypsin Susceptibility and Ninhydrin Assay
- To prepare genipin cross-linked L-PRF, rinse membranes with PBS and soak in 4 ml of 1% genipin solution (in 70% ethanol) for 48 hr. Rinse with PBS prior to experiments to remove excess genipin15, 16.
- Assess the stability of genipin crosslinking of L-PRF by its resistance to degradation by trypsin. Place L-PRF membrane (n=3) and genipin crosslinked L-PRF in 500 µl of 0.01% trypsin and incubated at 37 °C for 3 days with a daily change of trypsin.
- Weigh samples at day 1 prior to enzyme exposure and at day 3. The difference in start and end weight represents enzymatic degradation17.
- Quantify the amount of cross-linking in genipin treated L-PRF (G-PRF) by ninhydrin assay. First prepare the standard curve using glycine (1 mM-0.031 mM) curve to establish the relationship between free amino acid concentration (FAA) and absorbance.
- Heat PRF samples with 1 ml of 2% (w/v) ninhydrin for 15 min at 100 °C.
- Allow the solution to cool to RT and add 1.5 ml of 50% ethanol.
- Analyze the absorbance at 570 nm using a suitable spectrophotometer.
- Determine cross-linking percentage using the formula below15
7. MTS Cell Proliferation Assay
- Grow MC3T3 (mouse calvarial preosteoblasts) in Minimum Essential Medium –alpha modification (αMEM) in T-75 flasks until an 80% confluent monolayer is obtained.
- Prepare fresh, sterile L-PRF membrane (open the L-PRF tube inside the cell culture hood) and transfer the membrane onto a new cell culture dish.
- Aspirate media from the flask and rinse the monolayer with PBS, add 5 ml of 0.05% trypsin and place the flask in the 37 oC incubator for 5 min, pipette the contents of the flask into a centrifuge tube and centrifuge at 400 x g for 5 min.
- Decant the supernatant, gently tap the tube to break the cell pellet and re-suspend with 4 ml of fresh α MEM, dispense a mixture of cell suspension (50 µl) and trypan blue (50 µl) into the hemocytometer and count the number of cells
- Seed 4×105 cells within 10 mm glass cloning rings placed on top of L-PRF membranes to retain the cells within the membranes (rings can be removed after 24 hr).
- At day 4, rinse constructs with PBS thrice for 10 min.
- Add 1 ml of serum free media and 200 µl MTS reagent to each well and incubate for 2 hr at 37 °C.
- Measure absorbance from 200 µl aliquots at 490 nm.
The scanning electron microscope image of the L-PRF clot at different sections (top, middle and bottom) layer is illustrated in Figure 2. As can be seen, the top portion is composed predominantly of fibrin network with no cells. The middle layer is enriched with platelets with evidence of their activation and degranulation. The lower layer has a mixture of leukocytes and red blood cells entrapped within a fibrin matrix.
The mechanical properties were evaluated in two modes: uniaxial tensile testing and suture retention strength test. The results demonstrate viscoelastic behavior of L-PRF. Even though the elastic modulus is low (0.47 MPa), the membrane is tough (energy to break, 5 N·mm) and is capable of undergoing significant deformation (217%, Figure 3). Data from suture retention testing, an indicator of the ability of the membrane to be sutured to the tissues, suggested a significantly tough and deformable material (modulus-0.2 MPa, strain-140% and energy to break-3.2 N.mm) in L-PRF (Figure 4).
One of the limitations of fibrin products in regenerative medicine is its short biological life. Made from endogenous fibrin, L-PRF is susceptible to enzyme degradation and undergoes fibrinolysis. In order to evaluate the resistance of L-PRF to enzyme-mediated degradation, fresh L-PRF was subjected to trypsin treatment (0.01%) and incubated at 37 oC. We observed complete degradation of L-PRF within three days. Genipin crosslinking of L-PRF membranes decreased degradation by almost 60% (Figure 5).
The ability of L-PRF membranes to support cell growth was evaluated by culturing mouse calvarial osteoblasts on crosslinked and uncrosslinked membranes. Uncrosslinked clots underwent degradation to various levels while the genipin crosslinked membranes retained their structure and supported cell growth (Figure 6).
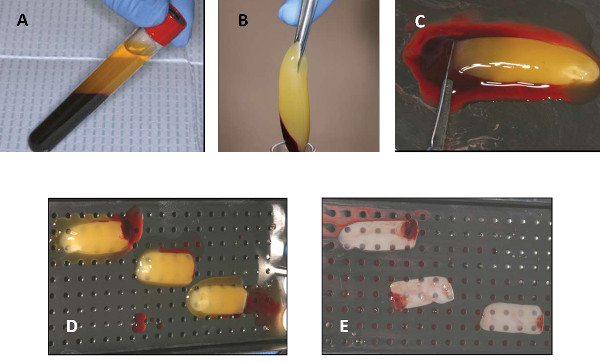
Figure 1. Steps in the generation of L-PRF. (A) After centrifugation of whole blood in a glass tube, three layers will be visible. (B) After decanting the PPP, the L-PRF is being removed using a sterile tweezers. (C) The red blood cell base is being scraped off using a scalpel and laid on a perforated metal tray (D). After gentle compression, the PPP is squeezed out and a firm L-PRF membrane is formed. Please click here to view a larger version of this figure.
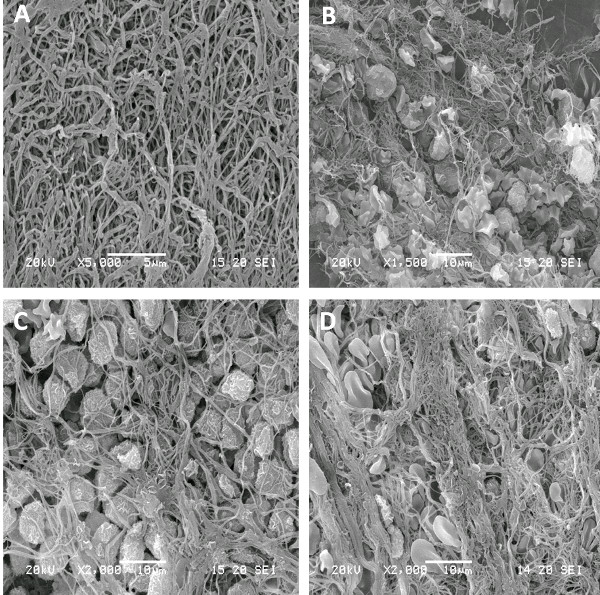
Figure 2. SEM image of different layers of fresh L-PRF. (A) represents the fibrin-rich layer; (B) is a zone of enriched platelets with various degree of activation; (C) is the buffy coat with numerous leukocytes and (D) is the red blood cell base. Please click here to view a larger version of this figure.
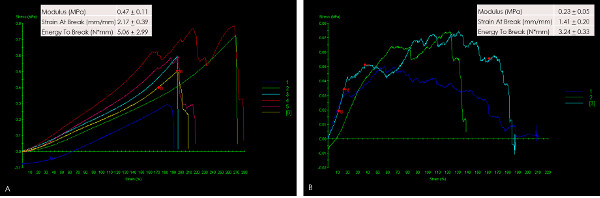
Figure 3. Stress-strain curves following mechanical loading of L-PRF in uniaxial tensile testing mode (A) and Suture retention strength (B). The loading pattern of each sample is represented in different color. The uniaxial tensile testing data (A) indicate a low modulus, a large elastic deformation and a rapid failure. Upon distension by a suture (B), L-PRF represents a membrane that is tough (area under the curve) as well as distensible. Good clustering of data suggests minimal variation between samples. Please click here to view a larger version of this figure.
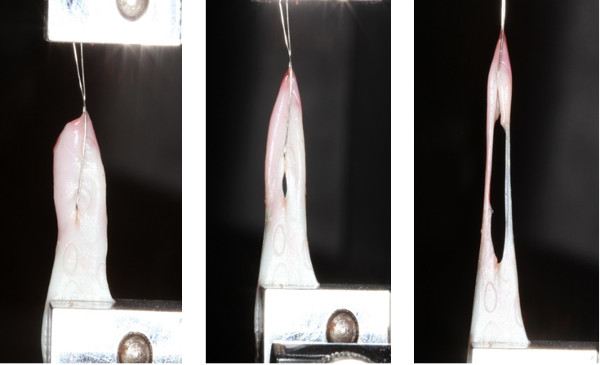
Figure 4. Photographs of actual failure in suture retention strength testing. A 220 µm thick stainless steel orthodontic ligature wire was passed through the middle of L-PRF and tied to the upper jaw member of the tensile testing machine. The other end was attached to the lower grip and stretched at a constant rate. Notice the elongation of the membrane and its resistance to tear, suggesting excellent resilience of L-PRF. Please click here to view a larger version of this figure.
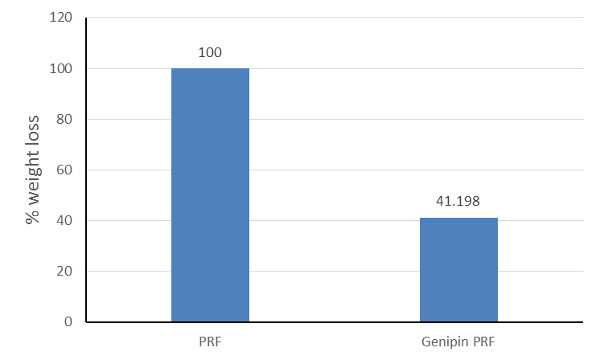
Figure 5. Degradation of L-PRF membranes following incubation in 0.01% trypsin. All L-PRF membranes disintegrated completely in trypsin within 3 days while genipin-crosslinked L-PRF were 60% more stable. This shows that chemical crosslinking can be a viable strategy to improve the longevity of L-PRF membranes when placed in vivo.
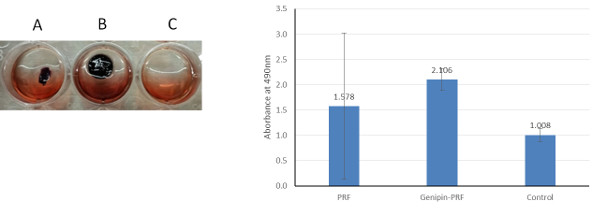
Figure 6. Effect of L-PRF crosslinking on cell viability. Representative images of 4 day culture of MC3T3 cells on uncrosslinked L-PRF (A), genipin-crosslinked L-PRF (B) and tissue culture plastic (C). Uncrosslinked L-PRF degraded in culture to variable extent and showed cell activity similar to plastic. Genipin crosslinked L-PRF maintained their structure and supported robust cell survival. To the right is quantified data (+SD) from independent experiments with three replicates. Please click here to view a larger version of this figure.
