Assessment and Communication for People with Disorders of Consciousness
Summary
With this experiment, one might be able to detect consciousness in people with disorders of consciousness. Furthermore, the approach can create a simple communication channel that enables people to give simple YES/NO answers to questions.
Abstract
In this experiment, we demonstrate a suite of hybrid Brain-Computer Interface (BCI)-based paradigms that are designed for two applications: assessing the level of consciousness of people unable to provide motor response and, in a second stage, establishing a communication channel for these people that enables them to answer questions with either 'yes' or 'no'. The suite of paradigms is designed to test basic responses in the first step and to continue to more comprehensive tasks if the first tests are successful. The latter tasks require more cognitive functions, but they could provide communication, which is not possible with the basic tests. All assessment tests produce accuracy plots that show whether the algorithms were able to detect the patient's brain's response to the given tasks. If the accuracy level is beyond the significance level, we assume that the subject understood the task and was able to follow the sequence of commands presented via earphones to the subject. The tasks require users to concentrate on certain stimuli or to imagine moving either the left or right hand. All tasks are designed around the assumption that the user is unable to use the visual modality, and thus, all stimuli presented to the user (including instructions, cues, and feedback) are auditory or tactile.
Introduction
The diagnosis of patients in Vegetative State (VS) or Minimal Conscious State (MCS) is difficult, and misclassifications often occur. A study in 2009 compared the accuracy of diagnosis between the clinical consensus versus a neurobehavioral assessment1. Out of 44 patients diagnosed with VS based on the clinical consensus of the medical team, 18 (41%) were found to be in MCS following a standardized assessment with the Coma Recovery Scale-Revised (CRS-R). This result is consistent with previous studies, which showed that 37 - 43% of patients diagnosed with VS demonstrated signs of awareness2,3. Classification scales are based on behavioral observations or on assessments of auditory, visual, verbal, and motor functions, as well as communication and arousal levels. New technologies that could add brain activity data are a perfect tool to overcome the restrictions imposed by behavioral rating scales. Patients may be able to modulate their brain responses despite being unable to produce the behavioral changes required for the rating scale. Monti et al.4 demonstrated that functional Magnetic Resonance Imaging (fMRI) could detect voluntary changes in blood oxygenation-level-dependent responses, which are related to imagining motor movements or spatial imagery tasks, in 5/54 patients diagnosed with a Disorder of Consciousness (DOC). Four of them had previously been classified to be in MCS. Thus, in a minority of cases, patients who meet the behavioral criteria for a vegetative state have residual cognitive function and even conscious awareness.
Electroencephalography (EEG)-based BCIs can also detect brain activity resulting from imagination or the attempt of motor movements. There are also other BCI paradigms that can determine whether a person can show awareness by voluntarily following a predefined task. EEG-based BCIs have other advantages relative to fMRI-based assessments. For example, EEG systems are much more cost effective and portable, and they can be easily used at the patient's bedside.The major noninvasive BCI approaches include Slow Cortical Potentials (SCPs), P300s, Steady-State Visual Potentials (SSVEPs), and Motor Imagery (MI). SCPs have provided low information transfer rates and require extensive training (see Wolpaw et al.)5, while SSVEPs require visual attention. Both approaches are therefore not used in this protocol. With a P300 speller, Ortner et al.5 reached an accuracy of 70% for disabled people. This number could eventually be increased. For example Turnip et al.7 improved their P300 classification accuracy by using an adaptive neural network classifier. For this protocol, we selected tactile and auditory P300 approaches in addition to the MI, because both of them can be used without vision, and each have unique advantages. MI can provide faster communication than a nonvisual P300 BCI, whereas P300 BCIs require very little training. Therefore, this hybrid BCI protocol can implement a whole suite of EEG-based BCI approaches for DOC patients. Furthermore, since the tasks are relatively quick and easy to repeat, different approaches could be explored repeatedly with each patient to decrease the number of incorrect classifications of DOC patients.
Four different BCI approaches were explored: (i) auditory P300, (ii) vibrotactile P300 with two stimulators, (iii) vibrotactile P300 with three stimulators, and (iv) MI.
The paradigm i auditory P300 approach uses an auditory oddball paradigm, in which deviant stimuli (1,000 Hz beeps) are randomly distributed within a train of more probable standard stimuli (500 Hz beeps). In paradigm ii, the stimuli are delivered via vibrotactile stimulators that are placed on the left and right wrists. The tactor on the left wrist delivers the standard stimuli, and the tactor on the right wrist deliver the deviant (target) stimuli. For paradigm iii, an additional stimulator is placed on the subject's right ankle, or on another location, such as the middle of the back. This stimulator delivers a train of standard stimuli, while the two stimulators on the left and right wrist both deliver deviant stimuli. To assess consciousness with the two vibrotactile paradigms, the subject is told via earphones to silently count each stimulus to one wrist while ignoring other stimuli. A random mechanism decides whether to choose the left or right wrist, and each run has four sets of 30 trials each, with a new target hand for each trial.
The following signal processing is done for paradigms i, ii, and iii: eight EEG channels are acquired using a sampling frequency of 256 Hz. The probability of a deviant stimulus is 1/8; hence, there will be seven standard stimuli for each deviant stimulus. Each run has 480 total stimuli. One run of paradigm i takes 7 min 20 s, while each run of paradigms ii and iii takes 2 min 30 s. If the patient silently counts each deviant stimulus, these stimuli elicit several Event-Related Potentials (ERPs), including the P300, a positive peak about 300 ms after stimulus onset. Each beep lasts 100 ms. For each stimulus trial, a window of 100 ms before and 600 ms after the beep is stored for signal processing. Data are then downsampled by a factor of 12, resulting in 12 samples for the 60 ms post-stimulus interval. Finally, all sample time channel features are entered into a linear discriminant analysis8, resulting in 12 x 8 = 96 features. To calculate the accuracy plot (Figure 1 & 2), the following procedure is repeated ten times, and the results are averaged into one single plot. The deviant and standard trials are randomly assigned into two equal-sized pools. One pool is used to train a classifier, and the other pool is used to test the classifier. The classifier is tested on an increasing number of averaged stimuli out of the test pool. At first, it is tested on only one deviant and seven standard stimuli. If the classifier detected the deviant stimulus correctly, the resulting accuracy is 100%, and it is 0% otherwise. The same is done for 2 averaged deviant stimuli and 14 averaged standard stimuli, for 3 deviant stimuli and 21 standard stimuli, and so on until the full test pool is used. This produces a plot of 30 single values (for 30 deviant stimuli in the test pool), each one either 100% or 0%. The averaging of 10 single plots results in values ranging from 0% to 100%. Increasing the number of averaged stimuli will increase the accuracy if the subject can follow the task, because the averaging of stimuli reduces random noise in the data. An accuracy significantly beyond chance level (12.5%) shows that a P300 response can be elicited in the subject and that a response in the subject's brain did appear.Paradigms i and ii can only be used to assess consciousness. If the accuracy reached during the assessment is higher than 40%, one can go on further to use the communication of paradigm iii or iv.
In the communication task of paradigm iii, the subject chooses to concentrate on the stimuli on the left-hand side if he/she wants to answer "YES" or on the right-hand side to answer "NO." The classifier detects which hand the user was concentrating on and presents the answer.
Paradigm iv records 120 trials, each of which lasts 8 s, separated by 1 s breaks.This results in 10 s x 120 = 18 min of overall session time. Paradigm iv uses 16 EEG channels distributed over the sensorimotor cortex. The sampling frequency is 256 Hz. Each trial begins with a cue, presented via earphones, that instructs the subject to imagine moving either the left or right hand. The sequence of left- and right-hand instructions is randomized. For signal preprocessing, the method of Common Spatial Patterns (CSP)10,12,13 is used. This method yields a set of spatial filters designed to minimize the variance of one class while maximizing variance for the other class. This results in four features, which are classified by the linear discriminant analysis8. The whole classification procedure is described in detail in a recent publication, showing a grand average classification accuracy of 80.7% after only 60 min of training in healthy users13. The calculation of accuracy is done via cross-validation. This refers to partitioning a sample of data into complementary subsets, performing the analysis on one subset (training pool), and validating the analysis on the other subset (testing pool). Before the separation of data into the pools, trials containing artifacts are rejected. A trial is considered to contain artifacts if the absolute value of the amplitude exceeds 100 µV at any time during the trial. The accuracy is calculated for all movements in the testing pool within a timeframe of 1.5 s after the attention beep until the end of the trial, in steps of 0.5 s. For each step and each trial, the classification result is either 100 or 0%. The accuracies of all trials of the test pool are then averaged for each single step, resulting in accuracy levels ranging between 0% and 100%. Finally, the average of ten repetitions of the cross-validation results is shown in the accuracy plot. Examples can be seen in Figures 3 & 4. The plots are separated for imaging movement in the left hand (yellow), right hand (blue), and all movements together (green). The horizontal line in magenta represents the confidence limit, which depends on the number of trials that were used for the analysis. This is the number of total trials minus the number of rejected trials. It shows the 95% confidence interval using the Clopper Pearson method9. An accuracy level above that line means that the result is statistically significant (alpha <0.05).
Protocol
All steps within this protocol are according to the principles of the declaration of Helsinki.
1. System Setup
- Using a USB cable, connect the amplifier to the computer running the software and turn on the amplifier.
- Connect the hardware dongle to a free USB slot in the computer.
NOTE: This is necessary to run the software. - Put the antistatic wrist band onto the subject's wrist and connect it to a free power plug.
NOTE: This band is designed to help ground the subject to the earth to reduce the noise that can influence the EEG quality. - Connect the driver box with the USB cable to a free slot of the computer.
- Connect the trigger cable to the driver box as follows:
- Connect the "g.STIMbox OUT 5"-labeled connector to "OUT 5" of the driver box.
- Connect the "g.STIMbox OUT 6"-labeled connector to "OUT 6" of the driver box.
- Connect the "g.STIMbox OUT 7"-labeled connector to "OUT 7" of the driver box.
- Connect the "g.USBamp DIO 1"-labeled connector to the "DIG I/O 1" socket of the g.USBamp.
- Connect the three tactors to OUT 1, OUT 2, and OUT 3 of the driver box.
- Connect the "TRIG OUT"-labeled connector to the "TRIG OUT" socket of the audio trigger adapter box.
- Take adhesive tape and fix one tactor on the left wrist, another one on the right wrist, and a third one on the right ankle.
- Connect a male/male audio connector cable to the audio output of the computer and to the socket of the audio trigger adapter box that is labeled "AUDIO IN." Turn on the audio trigger adapter box and check if the battery status LED is green.
- Start the software, observe a window called "Add physician." Type the title, name, institution, and department into the empty fields. Click on "Add" to open another window.
- Enter the patient's name, city, country, birthdate, and check-in date into the window.
- Click the green "+" button below the blue arrow in the bottom-right section of the program. Enter the text "First test" into the "Name" field and "Getting familiar with the software" into the empty "Details" field.
NOTE: It is necessary to enter information into all empty fields in order to proceed with the program. - Finally, click on the "Select this patient" button.
- Attach 16 EEG channels to the subject's head using an electrode cap. Use the positions: FC3, FCz, FC4, C5, C3, C1, Cz, C2, C4, C6, CP3, CP1, CPz, CP2, CP4, and Pz according to the extended international 10-20 system14. Place a reference electrode on the right earlobe and a ground electrode on the forehead.
- To properly position the cap on the subject's head, use a tape measure to measure the distance between the nasion and inion, as well as the distance between the left and right preauricular points. Ensure that the electrode in the vertex position, Cz, is at the midpoint of these two distances. Put on the electrode cap and align this measured position with the Cz position of the electrode cap. The electrode cap is now in the correct position.
- Connect the electrodes to the electrode connection box, following the setup described in step 1.12. Connect the electrode connection box to the biosignal amplifier and ensure that the amplifier and connection box are switched on.
- Inject enough electrode gel into the electrodes to create a connection between the skin and the electrodes.
2. Auditory P300 Assessment
- After entering the patient's information, click the "Auditory P300" button on the left side of the screen. Click the "Assessment" button on the bottom right to start the assessment run.
- Check the signal quality of the EEG. The image with the brain on the right side of the screen provides a color-coded guide to the signal quality of each electrode, with red for bad signal quality, yellow for acceptable signal quality, and green for good signal quality.
- Open the settings menu via the settings button and confirm that auditory beeps can be heard. Present these beeps with two different frequencies to the subject and explain the task, which is to count each of the high-frequency beeps.
- Put the earphones into the user's ears and click the start button.
- After the assessment run finishes, check the results page and the accuracy plot (Figures 1 & 2). If the accuracy level is below 40%, repeat the run.
NOTE: If the subject's accuracy is below 40%, then reliable communication is unlikely, at least with that paradigm and recording session. Nevertheless, assessments with other approaches and/or at different times could yield different results.
3. Vibrotactile P300 Assessment with 2 Stimulators
- Click the "Vibrotactile 2 Tactor" button on the left side of the screen; then, click the "Assessment" button on the bottom right to start the assessment run. Repeat step 2.2.
- Open the settings menu via the settings button to confirm that the vibrations of the tactors can be felt. Instruct the subject that he/she will feel vibrations on the left and right wrists. The task is to count the number of vibration stimuli on the left wrist. After the instructions, click the start button.
- When the assessment run has finished, check the results page and the accuracy plot. If the accuracy level is below 40%, repeat the run.
NOTE: If the subject's accuracy is below 40%, then reliable communication is unlikely, at least with that paradigm and recording session. Nevertheless, assessments with other approaches and/or at different times could yield different results.
4. Vibrotactile P300 Assessment with 3 Stimulators
- Click the button "Vibrotactile 3 Tactor" button on the left side of the screen and then click the "Assessment" button on the bottom right to start the assessment run.
- Repeat step 2.2. Open the settings menu via the settings button to confirm that the vibrations of the tactors can be felt.
- Instruct the subject that he/she will feel vibrations on the left and right wrists and on the right ankle and will hear the command "LEFT" or "RIGHT" via the headphones. Ask the subject to count the stimuli on the selected hand until the next command appears or the run is over.
NOTE: "LEFT" means that the subject should count the vibration stimuli on the left side, while the "RIGHT" instructs the subject to count the stimuli on the right wrist. - Plug the earphones into the subject's ears and click the start button.
- After finishing the assessment run, check the results page and the accuracy plot. If the accuracy level is below 40%, repeat the run.
NOTE: If the subject's accuracy is below 40%, then reliable communication is unlikely, at least with that paradigm and recording session. Nevertheless, assessments with other approaches and/or at different times could yield different results.
5. Vibrotactile P300 Communication with 3 Stimulators
- Click the "Vibrotactile 3 Tactor" button on the left side of the screen. Click the "Communication" button on the bottom to start the communication run.
- Repeat step 2.2. Open the settings menu via the settings button and confirm that the vibrations of the tactors can be felt. In the settings menu, select the classifier with the highest accuracy level. This is usually the classifier with the highest accuracy level as determined by the system.
- Instruct the subject that he/she will feel vibrations on the left and right wrists and on the right ankle. Instruct the subject that he/she will hear a question and is supposed to answer either "YES" or "NO." To answer "YES," ask the subject to count the stimuli on the left hand; to answer "NO," ask the subject to count the stimuli on the right hand.
- Ask the patient a question that could be answered with either "YES" or "NO." After that, click the "Start new question" button.
NOTE: When the sequence has finished, the software presents the answer. It could be "YES," "NO," or no answer (if the software was unable to accurately detect the brain patterns).
6. MI assessment
- Click the "Motor Imagery" button on the left side of the screen. Click the "Assessment" button on the bottom right to start the assessment run.
- Repeat step 2.2. Open the settings menu via the settings button and confirm that the audio commands can be heard via the earphones.
- Instruct the subject that he/she will hear a beep, followed by a command saying either "LEFT" or "RIGHT." Instruct the subject to try squeezing a ball with the left hand after the command "LEFT" and squeezing a ball with the right hand after the command "RIGHT." Ask the subject to stop imagining the squeezing as soon as the subject hears the command "RELAX."
NOTE: In total, 60 commands in randomized order will be played. - Have the run last for 8 min. Click the pause button after about 4 min, wait for about 1 min, and continue the run.
NOTE: The pause is designed to help the subject maintain concentration throughout the run. - After the assessment, check the results page and the accuracy plot ( Figures 3 and 4).
NOTE: If the accuracy level is below the significance level, repeat the run. If the accuracy remains below this significance level, then reliable communication is unlikely, at least with that paradigm and recording session. Nevertheless, assessments with other approaches and/or at different times could yield different results.
7. MI Communication
- Click the "Motor Imagery" button on the left side of the screen. Click the "Communication" button on the bottom left to start the communication run. Repeat step 2.2.
- Open the settings menu with the setting button and select the classifier with the highest classification accuracy.
- Instruct the subject my saying that after the beep he/she can provide an answer to the question that was asked previously. To say "YES," ask the patient to imagine squeezing a ball with the left hand. To say "NO," the patient should imagine squeezing a ball with the right hand.
- Ask the patient a question that could be answered with either "YES" or "NO." After that, click the "Start new question" button.
NOTE: When the sequence has finished, the software presents the answer (Figure 5). It could be either "YES" or "NO."
Representative Results
Figures 1 & 2 show results from two P300 assessment runs (paradigms i, ii, and iii). In Figure 1, the accuracy reached 100%; thus, the subject's brain clearly indicated successful task completion. In Figure 2, the accuracy fluctuates around the chance level of 12.5%. No reliable brain response to the task could be detected. When accuracy is poor, we recommend double-checking the EEG signal quality across all electrodes and connectors. A result with an accuracy level of 12.5% would also be seen if one does not acquire EEG but simply white noise. If the accuracy level increases with the number of trials but does not get higher than 40%, only a weak brain response was found. In this case, we recommend investigating artifacts in the signal using the raw data scope. We also recommend repeating the procedure on another day, at another time. The patient could be more responsive at another time and generate better results.
Figures 3 & 4 show representative results of paradigm iv. The significance level is marked with the magenta-colored line. The red vertical line marks the time of the command onset. Before the command appears (red vertical line), the accuracy is around 50% for both plots. At this time, the patient does not know if the command will be "LEFT" or "RIGHT" and thus cannot perform the correct motor imagination. In Figure 3, the accuracy increases after the command presentation to more than 90%. This means that the person was consciously aware, because he was able to follow the randomized commands. In Figure 4, the classification accuracy fluctuates around 50%. This means that the system was not able to detect MI following the presented commands. MI paradigms can be challenging in BCI research, since not all users are able to control an MI BCI without training, and a minority cannot attain control even with training11. Therefore, in this case, bad accuracy could simply mean that the patient is not able to control the BCI via MI, at least without training. Furthermore, we recommend checking the signal quality after a bad result, as described above.
Figure 5 shows the result of a communication run that could be done with paradigms iii and iv. The lens marks the detected answer, which is "YES" in this example. If the answer was no, the lens would move to "NO." If the system was unable to detect an answer, then the lens would stay in the middle of the two possible answers. If the lens stays in the middle of the answers, a bad classifier could have been chosen. We recommend trying another classifier in the setup window.
A long session could have exhausted the patient. To achieve better results with communication, it might be preferable to minimize assessments and proceed as quickly as possible to the steps described for communication. This would be steps 4 & 5 for tactile communication and 6 & 7 for MI communication.
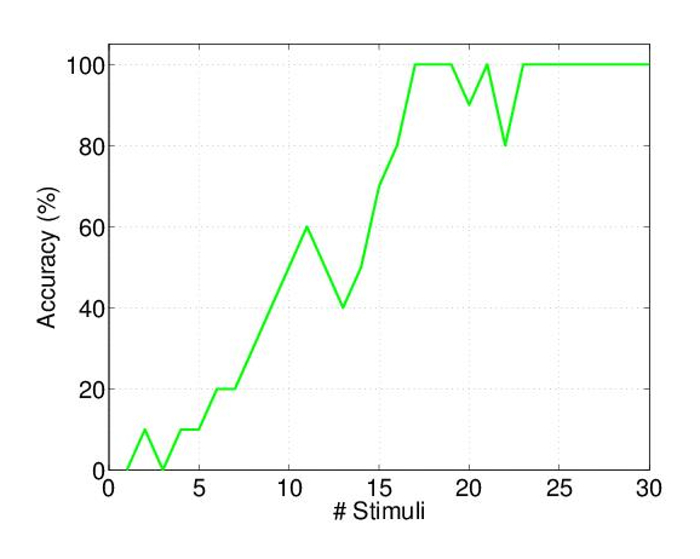
Figure 1. Accuracy Plot for Paradigms i, ii, & iii.
A good performance result in an accuracy, reaching 100%. Please click here to view a larger version of this figure.
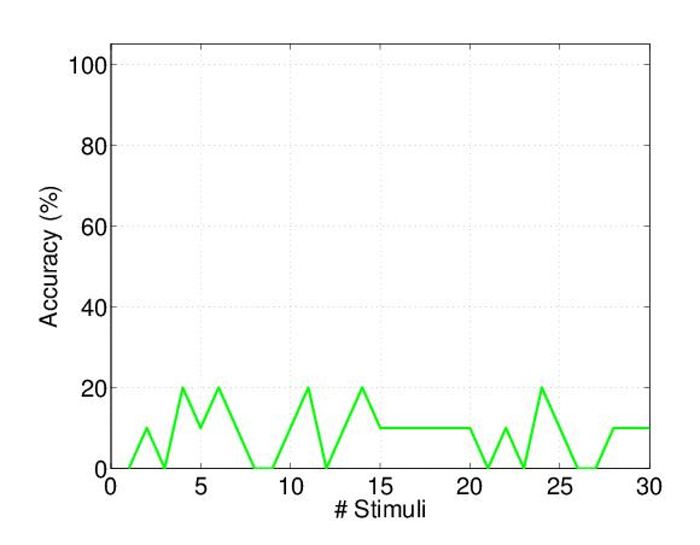
Figure 2. Another Accuracy Plot for Paradigms i, ii, & iii.
This time, no brain response could be detected by the system. Hence, the accuracy fluctuates around the chance level of 12.5%. Please click here to view a larger version of this figure.
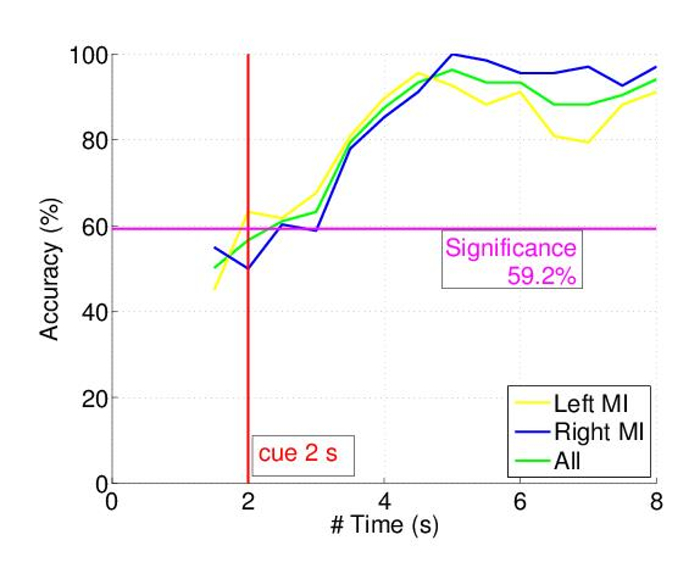
Figure 3. Accuracy Plot for Paradigm iv (MI).
The accuracy reaches above 90% in this example. Please click here to view a larger version of this figure.
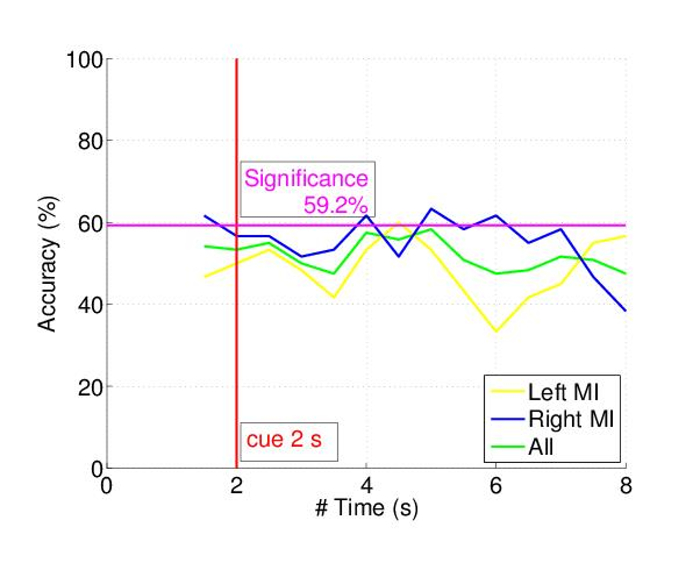
Figure 4. Accuracy Plot for Paradigm iv (MI).
No brain response could be detected by the system. Hence, the accuracy fluctuates around the chance level of 50%. Please click here to view a larger version of this figure.
Figure 5. Result of a Communication Task.
The lens marks the detected answer, "YES." Please click here to view a larger version of this figure.
Discussion
Prior research from numerous groups has shown that some DOC patients may exhibit conscious awareness through fMRI- or EEG-based assessments, even though assessments based on behavior suggest otherwise. Thus, there is a clear need for new systems and paradigms that can more accurately assess conscious awareness and even provide communication. Ideally, these systems should be inexpensive, portable, robust to noise in real-world settings, and easy to use (for both the patient and the system operator).
The protocols and system presented here serve two aims: to help assess the level of consciousness in persons with DOC and to establish a new communication channel for persons unable to communicate via speech, eye activity, or other tasks that require muscle control. The paradigms within the protocol are designed to test basic responses in the first steps. If the expected basic brain responses are detected, it is possible to go further and try the more complex paradigms, which are the vibrotactile P300 with three tactors and the MI. These two paradigms could be used also to establish a communication channel. EEG signal quality is critical in all of these protocols. Sometimes, EEG data cannot be distinguished from noise; some experience in EEG analysis is needed to recognize and manage noisy data.
Current standard assessment methods, in addition to being unreliable, are also time consuming and require a team of experts. Therefore, patients are often assessed only once, even though a patient's conscious awareness may fluctuate dramatically at different times. The protocol presented here could be easily repeated several times. Patients who do not exhibit conscious awareness might produce different results at another time. Also, a single assessment run could be done before each communication attempt to confirm that the subject is currently in a conscious state.
Another reason to implement different paradigms in the protocol is because some people may perform poorly with one paradigm but perform very well with another. Similarly, people might prefer one paradigm because it seems easier to them. After exploring different options with different paradigms, patients could choose the approach they prefer. This is consistent with the "hybrid" BCI approach, which supports providing multiple communication options to improve communication efficacy and user satisfaction.
The accuracy plots, in combination with the percentage level of correct classifications, yields an objective result that reflects how well the pattern recognition algorithm could discriminate the different brain states during the tasks. Therefore, no subjective interpretation of brain patterns or averaged responses is necessary.
The vibrotactile communication with three tactors was tested on group of six chronic locked-in patients15. They reached an average accuracy during communication of 55.3%, and all of them were above the chance level of 12.5%. The MI communication task was tested on a group of twenty healthy users13, showing an average accuracy of about 80%. Only one of the twenty persons had a control accuracy below chance level.
It is important to mention that a run or even a complete session with poor accuracy does not conclusively prove that there is no brain response or no consciousness within the subject. It just means that the system was unable to detect voluntary brain responses. This could occur due to poor signal quality, difficulty hearing or understanding task instructions, or simply because a minority of subjects cannot produce the desired EEG activity despite performing the task.
Consistent with prior work from our group and others, the presented work shows that it is advisable to assess the level of consciousness in patients suffering from DOC with brain imaging techniques. fMRI is also a useful technique to track the patient's current brain activity. It was shown that oddball paradigms that elicit evoked potentials, as well as motor imagery and other tasks, can produce hemodynamic responses that could be tracked by fMRI17,18. Compared to fMRI, the EEG has notable advantages: EEG-based tools can be applied at bedside, without equipment that is expensive and non-portable and requires considerable expertise. Transporting the patient to the scanner and the acoustic noise from the scanner can both be stressful for the patient. Near infrared spectroscopy (NIRS) is portable and can have slightly better spatial resolution than EEG, but it has worse temporal resolution19. NIRS is suitable to monitor MI20,21, but not for evoked potentials. For example, Naseer and Hong22 demonstrated high-classification accuracy for MI-BCI using fNIRS. With trials that each lasted 50 s, they achieved 77.35% for left-hand MI and 83% for right-hand MI. With EEG-based BCIs, Guger et al.23 found that about 20% of 99 sessions reached an accuracy above 80% and a further 70% of the 99 sessions reached an accuracy above 60%. Ortner et al. showed an average peak accuracy of about 80% using the CSP method. This method needs more EEG electrodes than the ones used from Guger and colleagues, but it results in higher accuracy rates. Using the CSP method, Ramoser et al.23 demonstrated that an increase of electrodes from 18 – 56 does not significantly improve the performance; we therefore conclude that the chosen number of 16 electrodes in our method is sufficient. Recently, Coyle et al. used CSP for classifying and training MI in DOC patients16. All four subjects demonstrated significant and appropriate brain activation during the assessment.
Assessing MI through a hybrid NIRS-EEG BCI could result in high classification accuracy, as Khan et al.20 showed. This could be a promising future direction, although an additional neuroimaging tool increases the complexity and costs of the device.
The protocol presented here provides a relatively easy tool to assess brain responses within the EEG signal of DOC patients. Interpreting these classification results and implementing any changes to medication, therapy, or other medical treatments still requires medical experts. Future directions of this method could be more advanced stimulation techniques using a higher number of degrees of freedom. For example, instead of offering tools to only say "YES" or "NO," future devices could allow more possible answers to one question. In a further step, one could also use context-based answers. For example, if the patient has a music player running, one could offer the possibility to control the sound level or switch to the next song. Also, the MI paradigm needs to be tested in DOC patients.
Disclosures
The authors have nothing to disclose.
Acknowledgements
This work was supported by the European Union FP 7 project DECODER and the European Union ODI Project COMAWARE.
Materials
| g.USBamp | g.tec medical engineering GmbH | 1 | Biosignal amplifier |
| Power supply | GlobTek Inc. | 1 | Medical mains power supply for the g.USBamp |
| USB cable | g.tec medical engineering GmbH | 1 | Connects the g.USBamp to the computer |
| EEG electrodes gSCARABEO | g.tec medical engineering GmbH | 16 | Active EEG electrodes |
| EEG electrode gSCARABEOgnd | g.tec medical engineering GmbH | 1 | passive ground electrode |
| EEG electrode g.GAMMAearclip | g.tec medical engineering GmbH | 1 | active reference electrode |
| g.GAMMAbox | g.tec medical engineering GmbH | 1 | Connects the amplifier to the EEG electrodes |
| g.USBampGAMMAconnector | g.tec medical engineering GmbH | 1 | Connects the g.GAMMAbox to the g.USBamp |
| EEG cap | g.tec medical engineering GmbH | 1 | To position electrodes |
| Computer | Hewlett-Packard | 1 | To run the software. Alternatively computers from other manufacturers could be used. |
| g.VIBROstim | g.tec medical engineering GmbH | 3 | Tactors for sensory stimulation |
| Audio trigger adapter box | g.tec medical engineering GmbH | 1 | To split up the audio signal into audio commands for the headphones and trigger signals. This box connects to the amplifier. |
| Anti static wrist band | g.tec medical engineering GmbH | 1 | To suppress noise in the EEG |
| Trigger cable | g.tec medical engineering GmbH | 1 | To connect the audio trigger adapter box and the g.STIMbox to the g.USBamp |
| Audio connector cable | g.tec medical engineering GmbH | 1 | Audio cable to connect the audio trigger adapter box to the computer |
| Hardlock | g.tec medical engineering GmbH | 1 | To run the software |
| SE215-K | Shure Europe GmbH | 1 | Noise suppressing earphones. Alternatively other earphones could be used. |
| g.STIMbox | g.tec medical engineering GmbH | 1 | Driver box for tactile stimulators |
| mindBEAGLE software | g.tec medical engineering GmbH | 1 | software package |
| g.GAMMAgel | g.tec medical engineering GmbH | 1 | conductive electrode gel |
References
- Schnakers, C., Vanhaudenhuyse, A., et al. Diagnostic accuracy of the vegetative and minimally conscious state: Clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 9, (2009).
- Childs, N. L., Mercer, W. N., Childs, H. W. Accuracy of diagnosis of persistent vegetative state. Neurol. 43 (8), 1465-1465 (1993).
- Andrews, K., Murphy, L., Munday, R., Littlewood, C. Misdiagnosis of the vegetative state: retrospective study in a rehabilitation unit. Bmj. 313 (7048), 13-16 (1996).
- Monti, M. M., Vanhaudenhuyse, A., et al. Willful modulation of brain activity in disorders of consciousness. New England Journal of Medicine. 362 (7), 579-589 (2010).
- Wolpaw, J. R., Birbaumer, N., McFarland, D. J., Pfurtscheller, G., Vaughan, T. M. Brain-computer interfaces for communication and control. Clinical Neurophysiology. 113, 767-791 (2002).
- Ortner, R., Aloise, F., et al. Accuracy of a P300 Speller for People with Motor Impairments: a Comparison. Clinical EEG and Neuroscience. 42 (4), 214-218 (2011).
- Turnip, A., Hong, K. -. S. Classifying mental activities from EEG-P300 signals using adaptive neural network. Int. J. Innov. Comp. Inf. Control. 8 (9), 6429-6443 (2012).
- Lugger, K., Flotzinger, D., Schlögl, A., Pregenzer, M., Pfurtscheller, G. Feature extraction for on-line EEG classification using principal components and linear discriminants. Med. Biol. Eng. Comput. 36 (3), 309-314 (1998).
- Johnson, N. L., Kemp, A. W., Kotz, S. . Univariate discrete distributions. 444, (2005).
- Guger, C., Ramoser, H., Pfurtscheller, G. Real-Time EEG Analysis with Subject-Specific Spatial Patterns for a Brain-Computer Interface (BCI). IEEE Trans. Rehab. Eng. 8, 447-456 (2000).
- Vidaurre, C., Blankertz, B. Towards a Cure for BCI Illiteracy. Brain Topography. 23 (2), 194-198 (2010).
- Blankertz, B., Tomioka, R., Lemm, S., Kawanabe, M., Müller, K. -. R. Optimizing Spatial Filters for Robust EEG Single-Trial Analysis. IEEE Signal Process. Mag. 25 (1), 41-56 (2008).
- Ortner, R., Scharinger, J., Lechner, A., Guger, C. How many people can control a motor imagery based BCI using common spatial patterns. Proceedings of the 7th Annual International IEEE EMBS Conference on Neural Engineering. , (2015).
- Chatrian, G. Ten percent electrode system for topographic studies of spontaneous and evoked EEG activity. Am J Electroencephalogr Technol. 25, 83-92 (1985).
- Lugo, Z. R., Rodriguez, J., et al. A vibrotactile p300-based brain-computer interface for consciousness detection and communication. Clin. EEG Neurosci. 45 (1), 14-21 (2014).
- Coyle, D., Stow, J., McCreadie, K., McElligott, J., Carroll, &. #. 1. 9. 3. ;. Sensorimotor Modulation Assessment and Brain-Computer Interface Training in Disorders of Consciousness. Archives of Physical Medicine and Rehabilitation. 96 (3), 62-70 (2015).
- Kiehl, K. A., Laurens, K. R., Duty, T. L., Forster, B. B., Liddle, P. F. Neural sources involved in auditory target detection and novelty processing: an event-related fMRI study. Psychophysiology. 38 (1), 133-142 (2001).
- Opitz, B., Mecklinger, A., Cramon, D., Kruggel, F. Combining electrophysiological and hemodynamic measures of the auditory oddball. Psychophysiology. 36 (1), 142-147 (1999).
- Min, B. -. K., Marzelli, M. J., Yoo, S. -. S. Neuroimaging-based approaches in the brain-computer interface. Trends in Biotechnology. 28 (11), 552-560 (2010).
- Khan, M. J., Hong, M. J., Hong, K. -. S. Decoding of four movement directions using hybrid NIRS-EEG brain-computer interface. Frontiers in Human Neuroscience. 8, (2014).
- Naseer, N., Hong, K. -. S. fNIRS-based brain-computer interfaces: a review. Frontiers in Human Neuroscience. 9, (2015).
- Naseer, N., Hong, K. -. S. Classification of functional near-infrared spectroscopy signals corresponding to the right- and left-wrist motor imagery for development of a brain-computer interface. Neuroscience Letters. 553, 84-89 (2013).
- Guger, C., Edlinger, G., Harkam, W., Niedermayer, I., Pfurtscheller, G. How many people are able to operate an EEG-based brain-computer interface (BCI)?. Neural Systems and Rehabilitation Engineering, IEEE Transactions on. 11 (2), 145-147 (2003).
- Ramoser, H., Mueller-Gerking, J., Pfurtscheller, G. Optimal spatial filtering of single trial EEG during imagined hand movement. IEEE Transactions on Rehabilitation Engineering. 8 (4), 441-446 (2000).
