The Monoiodoacetate Model of Osteoarthritis Pain in the Mouse
Summary
Osteoarthritis (OA), or degenerative joint disease, is a debilitating condition associated with pain that remains only partially controlled by available analgesics. Animal models are being developed to improve our understanding of OA-related pain mechanisms. Here we describe the methodology for the monoiodoacetate model of OA pain in the mouse.
Abstract
A major symptom of patients with osteoarthritis (OA) is pain that is triggered by peripheral as well as central changes within the pain pathways. The current treatments for OA pain such as NSAIDS or opiates are neither sufficiently effective nor devoid of detrimental side effects. Animal models of OA are being developed to improve our understanding of OA-related pain mechanisms and define novel pharmacological targets for therapy. Currently available models of OA in rodents include surgical and chemical interventions into one knee joint. The monoiodoacetate (MIA) model has become a standard for modelling joint disruption in OA in both rats and mice. The model, which is easier to perform in the rat, involves injection of MIA into a knee joint that induces rapid pain-like responses in the ipsilateral limb, the level of which can be controlled by injection of different doses. Intra-articular injection of MIA disrupts chondrocyte glycolysis by inhibiting glyceraldehyde-3-phosphatase dehydrogenase and results in chondrocyte death, neovascularization, subchondral bone necrosis and collapse, as well as inflammation. The morphological changes of the articular cartilage and bone disruption are reflective of some aspects of patient pathology. Along with joint damage, MIA injection induces referred mechanical sensitivity in the ipsilateral hind paw and weight bearing deficits that are measurable and quantifiable. These behavioral changes resemble some of the symptoms reported by the patient population, thereby validating the MIA injection in the knee as a useful and relevant pre-clinical model of OA pain.
The aim of this article is to describe the methodology of intra-articular injections of MIA and the behavioral recordings of the associated development of hypersensitivity with a mind to highlight the necessary steps to give consistent and reliable recordings.
Introduction
Clinically, osteoarthritis (OA), or degenerative joint disease, is a painful and debilitating condition characterized by a progressive loss of articular cartilage, mild inflammation of the tissues in and around the joints, and sometimes formation of osteophytes and bone cysts. Patients with OA report persistent pain 1 and display increased sensitivity to pressure and noxious stimuli in the arthritic joint 2-4. At present, there is no cure for OA with available therapeutic approaches and analgesics are prescribed to alleviate the pain associated with this condition, with some degree of success5. However, OA pain remains a clinical issue and animal models of OA are being developed to improve our understanding of OA-related pain mechanisms and disclose novel targets for therapy.
There are several animal models of OA available with different characteristics 6. Surgical methods, such as anterior cruciate ligament transection, can be utilized. However, they involve skillful surgical intervention and are primarily performed in the rat, while destabilization of medial meniscus (DMM) is used in the mouse. Spontaneous development of OA occurs in guinea pig and spontaneous joint degeneration has been reported in C57 black mice from 3 to 16 months of age 7,8. Spontaneous OA models do not involve any intervention to induce the condition, but they have inherent variability, and as such, incur greater numbers and cost 9,10. Chemically induced models, on the other hand, require much less invasive procedures than surgical models, and as such, are easier to implement and permit the study of OA lesions at different stages. These models include single injections in the knee of inflammatory agents, immunotoxins, collagenase, papain, or monoiodoacetate, which can be toxic if they escape the joint space. Of all chemical models of OA, MIA is the one most often used, particularly to test the efficacy of pharmacologic agents to treat pain, as this model generates a reproducible, robust, and rapid pain-like phenotype that can be graded by altering MIA dosage 11-15.
Intra-articular injection of MIA in rodents reproduces OA-like lesions and functional impairment that can be analyzed and quantified. MIA is an inhibitor of glyceraldehyde-3-phosphatase, disrupting cellular glycolysis and eventually resulting in cell death 16,17. Intra-articular injection of MIA causes chondrocyte cell death, leading to cartilage degeneration and subsequent subchondral bone alterations such as appearance of bone osteophytes 18,19.
As the utility of MIA in the rat has been described before 20, in this paper we focus on the methodology of MIA-induced OA in mice as this model is being increasingly used with the availability of knock-out mice. We describe a procedure for the injection of very small volumes into the knee and methods for measuring sensitivity to noxious and non-noxious stimuli in the hind limbs.
The breakdown of the methodology will help to reduce variability, and as such, refine the model and reduce the number of animals needed for study.
Protocol
Procedures involving animal subjects have been approved by the Ethical Committee at King's College London and are in accordance with UK Home Office Regulations (Animals Scientific Procedures Act 1986).
1. Intra-articular Injection of Monoiodoacetate in the Knee
- House 8 – 10 week-old mice in groups of 5 under a 12 hr light/dark cycle (lights on at 7:00 AM) with food and water ad libitum. Let the mice acclimatize for 1 week prior to starting the experiment.
- Randomize and cage mice in groups of 5. Use animal numbers as codes to blind the experimenter to treatments. Use body weights as parameters for randomization.
- On the day of injection, freshly prepare the solution of monoiodoacetate in sterile saline (0.9% NaCl) at the desired concentrations. Use sterile saline for injections in a separate group of control mice. The highest recommend dose of MIA is 1 mg in 10 µl.
Caution: Monoiodoacetate is very toxic. Therefore, it is recommended that gloves and mask are worn when handling the powder and preparing the solution. The solution should be sterile filtered with a 0.22 μm filter. - Anesthetize mice using an anesthetic trolley by first placing them in a chamber delivering 2% isoflurane in O2 mixture (flow rate 1.5 L/min) and then transfer mice to the nose cone section, which also delivers the 2% isoflurane-O2 mixture, and as such, maintains anesthesia during injection. Place vet ointment on the eyes to avoid their drying out while under anesthesia. Wear surgical gown, gloves, and mask while performing injection procedure.
- Confirm anesthesia by checking the animal's lack of response to a pinch stimulus on the hind paws.
- Once the animal is under anesthesia, place it on its back. Trim and wipe the area surrounding the knee joint with alcohol. Povidone iodine or chlorhexidine can be used as well for disinfection. The patellar tendon (white line bellow the patella) will become visible.
- In order to stabilize the injection site, keep the knee still, in a bent position, by placing the index finger beneath the knee joint and the thumb above the anterior surface of the ankle joint. Joint preference is not required.
- To find the precise site of injection, run a 26 G needle attached to a syringe horizontally along the knee (so as not to pierce the skin with the tip) until it finds the gap beneath the patella. Apply gentle pressure to mark the area and then lift the needle and syringe vertically for the injection. Insert the needle in the marked area, through the patellar tendon, perpendicular to the tibia. No resistance should be felt.
- Use thumb as a guide and inject superficial to the site of entry. After injection, massage the knee to ensure even distribution of the solution. Discard the needle immediately in the sharps bin.
- Place mice back into a clean home cage on a heated mat and allow them to recover. Keep constant vigilance on the animals until they regain suitable consciousness, which is measured by them regaining sternal recumbency. Once animals are recovered, return to their cage.
Note: It is suggested for best practice and training purposes that a dye is used and immediate post-mortem dissection performed to confirm correct localization of injection.
2. Measurement of Mechanical Hypersensitivity (Allodynia)
Note: Static mechanical withdrawal thresholds are assessed by applying von Frey hairs to the plantar surface of the hind paw.
- Bring mice to the behavioral room and let unrestrained animals acclimatize in acrylic cubicles (8 cm x 5 cm x 10 cm) atop a wire mesh grid.
- Train mice by handling and 2 hr habituation to the cubicles for two days prior to von Frey hair application in order to limit stress and ambulation during application of von Frey hairs. On test days, habituate animals to the cubicles for up to 60 min prior to testing. Wear gowns, gloves, and masks during all behavioral experiments.
- Apply calibrated von Frey hairs (flexible nylon fibers of increasing diameter that exert defined levels of force as calibrated by the manufacturing company and expressed as grams (g)) to the plantar surface of the hind paw until the fiber bends. Use 0.008, 0.02, 0.04, 0.07, 0.16, 0.4, 0.6, and 1.0 g fibers during testing.
- Hold each hair in place for 3 sec or until the paw is withdrawn, the latter defining a positive response. Starting with a stimulus strength of 0.07 g, apply hairs according to the "up-down method"21: mark as X a withdrawal response and O an absence of response. Apply in ascending order of force, up to 1 g (cut-off force), until a response is detected.
- Re-test the paw by repeating step 2.2.1, starting with the filament that exerts a force below the one that produced a withdrawal.
- Then, apply the remaining filaments sequentially, by descending force, until no withdrawal occurs. Re-apply filaments in ascending order until a response is observed. Continue until a sequence of six responses is obtained (e.g., OXOXOX), in order to obtain the 'k' value by referring to tabular values 21.
- Express paw withdrawal values as 50% paw withdrawal thresholds in grams. Use the formula (10[Xr + Kδ])/10,000 where Xr = value of last von Frey filament used in the sequence (in log units), k = tabular value, and δ = mean difference in forces between fibers. Where no response is detected, use the maximal response of 1 g 21,22.
- Following the procedure described above (2.2.1-2.2.4), assess mechanical thresholds of both hind paws before MIA injection as baseline values. After injection, assess thresholds of the ipsilateral and contralateral paws at regular day intervals for several weeks after MIA to ascertain the development of mechanical allodynia.
Note: For example, we report thresholds measured 0, 3, 5, 7, 10, 14, 21, and 28 days after MIA injection. Animals are considered allodynic when they display a response to 0.1 g or less. Normal responses fall within 0.6 – 1 g range.
3. Measurement of Weight Bearing Deficit
Note: Changes in weight bearing are measured using a weight incapacitance tester.
- Train each mouse to walk into a Plexiglass chamber on the apparatus and sit in the holding box. Place the mouse in front of the holding box, lift the entrance up 45°, and allow the mouse to walk in and close the box. Allow the animals to move freely until they adopt a sitting posture. This training takes at least two days and guarantees that the animal is still and not leaning on either side of the chamber. Calibrate the instrument before use with a 100 g check weight (or according to equipment instruction).
- Make sure that each hind paw is placed on the appropriate recording pad 11. The duration of each measurement takes 1 sec, as per the manufacturer's instructions.
- Collect three measurements of the weight borne on each hind paw from the recording pad for each recording session and use the mean value to calculate the difference in weight borne by ipsilateral and contralateral paws. Express values as the difference between contralateral and ipsilateral paws in grams.
- Assess weight bearing changes before MIA injection as baseline values. Then, repeat assessments at regular intervals over several weeks to ascertain the development of gate changes. For example, we report thresholds measured on 0, 3, 5, 7, 10, 14, 21, and 28 days after MIA injection.
Note: A normal weight bearing value of 50% represents an equal weight distribution across ipsilateral and contralateral hindlimb. Animals considered hypersensitive display a weight bearing change of approximately 45%. Measurements of mechanical thresholds and weight bearing deficits can be performed in the same mice, as neither end point affects the other. For pharmacological assessment, each group of animals should be tested at set times after dosing in line with the pharmacokinetic profile of the compound used.
Representative Results
We have recently reported that the injection of 0.5 – 1 mg MIA in the mouse knee joint induces referred mechanical hypersensitivity (allodynia) in the ipsilateral hind paw and weight bearing deficits for up to 4 weeks, although onsets are dose-dependent 23.
The data reported in Figure 1 constitute an example of the time course of MIA-induced mechanical hypersensitivity in the ipsilateral hind paws following a range of doses injected in the knee. Specifically, the lowest dose of MIA (0.5 mg/mouse) induced a 50% decrease of thresholds compared to the injection of saline on day 10, and thresholds decreased to 70% of those of saline controls by day 28 after injection. The intermediate dose of 0.75 mg of MIA resulted in a gradual decrease in thresholds that were 80% lower than saline control thresholds on day 10 and remained low up to day 28. The highest dose of 1 mg MIA was associated with a significant drop in threshold on day 5 and a further decrease on day 10, which was sustained up to day 28.
The data reported in Figure 2 provide examples of weight bearing changes that are associated with MIA injection in the knee joints. In this set of experiments, while the 0.5 mg MIA dose did not induce significant changes in weight bearing throughout the 28 day duration of the study, the 0.75 mg MIA dose resulted in a significant reduction in the weight borne by the ipsilateral paw from day 10 onwards. Notably, weight bearing asymmetry associated with 0.75 mg of MIA may produce variable and inconsistent results between studies 23. Instead, the dose of 1 mg MIA generally induces reproducible weight bearing asymmetry and the data in Figure 2 demonstrate significant reduction of weight borne on the ipsilateral hind paw from day 3 until the end of the observation period. As expected, saline-treated animals showed no weight bearing changes.
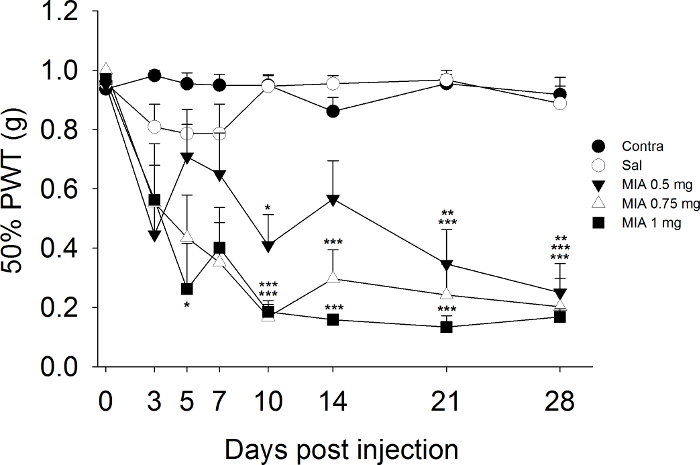
Figure 1. Development of Mechanical Allodynia Post MIA Injection. Paw withdrawal thresholds of the ipsilateral and contralateral hind paws were assessed before and after injection of MIA (0.5, 0.75, and 1mg/mouse) and saline (0.9% NaCl), n = 8 – 10 mice/group. *P<0.05, **P<0.01, ***P<0.001 versus saline-treated group; Two-way repeated measurements ANOVA followed by Student Newman-Keuls post hoc test. Please click here to view a larger version of this figure.
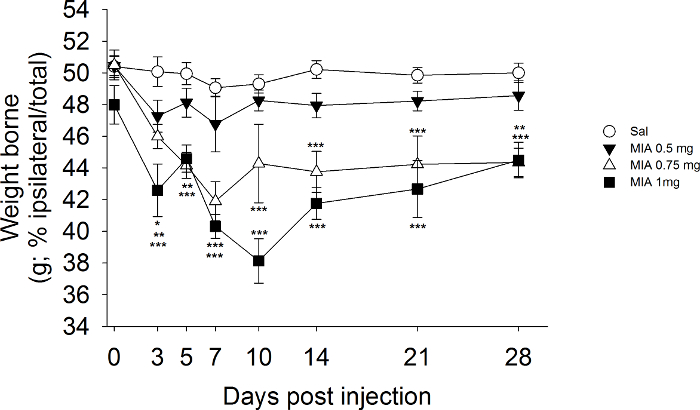
Figure 2. Development of Weight Bearing Deficits Post MIA Injection. Changes in body weight distribution between the two hind limbs were calculated as [(weight borne on ipsilateral paw / sum of the weight borne on the ipsilateral and contralateral paws)*100] were assessed before and after injection of MIA (0.5, 0.75, and 1 mg/mouse) and saline (0.9% NaCl), n = 8 – 10 mice/group. *P<0.05, **P<0.01, ***P<0.001 versus saline-treated group. Two-way repeated measurements ANOVA followed by Student Newman-Keuls post hoc test. Please click here to view a larger version of this figure.
Discussion
With this methodology, we describe a preferred method for inducing OA-like pain in the mouse by an intra-articular injection of MIA in a knee joint and assessment of sensitivity to non-noxious and noxious stimuli in the hind limbs. MIA injection is associated with persistent pain behavior, namely altered hind limb weight bearing and development of referred mechanical hypersensitivity (allodynia). Such static measurements can be complemented by gait analysis on a treadmill or by catwalk analysis in freely moving animals. MIA models are responsive to conventional pain-relieving therapies 24, indicating that they may be useful for discerning therapeutic approaches. While the injection of MIA is not technically difficult, the joint capsule can be pierced during the injection, resulting in leakage of MIA outside the capsule, and subsequent failure to induce toxicity of chondrocytes. Indeed, systemic injection of MIA can be fatal in rodents and possible effects of MIA on tissues and cells other than chondrocytes may confound results, besides being undesirable. As such, it must be stressed that great care needs to be given to the injection of the MIA, as it is a critical component of the model, and confidence needs to be given that the injection occurs into the articular space. This protocol helps to achieve that.
The protocols described here aim to ensure the animals provide consistent pain-like responses throughout the test period. Also, they allow adjustment of disease severity by altering the dose of MIA used to induce the pathology 15,23. The rapid induction of both disease state and pain-like behavior allow timely evaluation of pain-modifying compounds. This is advantageous over existing surgical and spontaneously developing models of OA, which can take a longer period of time to develop hypersensitivity. Also, particularly for the spontaneous models, the disease pathology does not manifest in all animals (approximately 20 – 80% 7), whereas the MIA model is associated with significant incidence of responders. Furthermore, spontaneous models are not suitable for measurements of changes in weight bearing, as OA develops in both knees. When considering behavioral measurements, the animals need to be kept calm and relaxed during the assessments. This is achieved, as detailed in the protocol, by early training before recording measurements and by repetitive handling, which allows animals to become familiar with the experimenter. A key point to reduce stress is to use the same experimenter for the behavioral test throughout, as constant changing will induce the issues previously mentioned. Like any model, the MIA model of OA bears limitations, such as the rapidity of joint disruption, which does not resemble the slow development of OA pathology in patients. One way to overcome this issue would be to complement this model with a surgical model of OA. The use of the MIA chemical model in compound development allows for the use of preventative and therapeutic protocols over the development and maintenance of OA-like pain. Finally, the MIA model would complement studies of phenotypical traits of knock-out mice, helping to further understand the OA disease.
Disclosures
The authors have nothing to disclose.
Acknowledgements
JSV is supported by a collaborative grant to MM by the European Commission (GAN 603191-PAINCAGE).
Materials
| Monoiodoacetate | Sigma-Aldrich | I-2512-25G | ||
| 0.9% Saline | Mini-Plasco basic | 365 4840 | ||
| Isoflurane | Merial | DNI 4090/1 | ||
| 26g Needle | Fisher Scientific | 12947606 | ||
| 50ul Hamilton Syringe | Sigma-Aldrich | 20701 | ||
| Von Frey Hairs | Linton Instruments | NC 122775-99 | ||
| Incapacitance tester | Linton Instruments | Delivery on Request | ||
| Testing Cage Rack | Ugo Basile | 37450 | ||
| Compact Anesthetic system | Vet -Tech | AN001B | ||
| Medical O2 | BOC | 101-F | ||
| Aldasorbers | Vet -Tech | AN006A | ||
References
- Farrell, M., Gibson, S., McMeeken, J., Helme, R. Pain and hyperalgesia in osteoarthritis of the hands. J. Rheumatol. 27 (2), 441-447 (2000).
- Kuni, B., Wang, H., Rickert, M., Ewerbeck, V., Schiltenwolf, M. Pain threshold correlates with functional scores in osteoarthritis patients. Acta. Orthop. 86 (2), 215-219 (2015).
- Wylde, V., Hewlett, S., Learmonth, I. D., Dieppe, P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 152 (3), 566-572 (2011).
- Wylde, V., Palmer, S., Learmonth, I. D., Dieppe, P. Test-retest reliability of Quantitative Sensory Testing in knee osteoarthritis and healthy participants. Osteoarthr. Cartil. 19 (6), 655-658 (2011).
- Hunter, D. J. Pharmacologic therapy for osteoarthritis–the era of disease modification. Nat. Rev. Rheumatol. 7 (1), 13-22 (2011).
- Lampropoulou-Adamidou, K., et al. Useful animal models for the research of osteoarthritis. Eur. J. Orthop. Surg. Traumatol. 24 (3), 263-271 (2014).
- Yamamoto, K., Shishido, T., Masaoka, T., Imakiire, A. Morphological studies on the ageing and osteoarthritis of the articular cartilage in C57 black mice. J. Orthop. Surg. (Hong Kong). 13 (1), 8-18 (2005).
- Huebner, J. L., Hanes, M. A., Beekman, B., TeKoppele, J. M., Kraus, V. B. A comparative analysis of bone and cartilage metabolism in two strains of guinea-pig with varying degrees of naturally occurring osteoarthritis. Osteoarthr. Cartil. 10 (10), 758-767 (2002).
- Thysen, S., Luyten, F. P., Lories, R. J. Targets, models and challenges in osteoarthritis research. Dis Model Mech. 8 (1), 17-30 (2015).
- Longo, U. G., et al. Osteoarthritis: new insights in animal models. Open. Orthop. J. 6, 558-563 (2012).
- Bove, S. E., et al. Weight bearing as a measure of disease progression and efficacy of anti-inflammatory compounds in a model of monosodium iodoacetate-induced osteoarthritis. Osteoarthr. Cartil. 11 (11), 821-830 (2003).
- Pomonis, J. D., et al. Development and pharmacological characterization of a rat model of osteoarthritis pain. Pain. 114 (3), 339-346 (2005).
- Schuelert, N., McDougall, J. J. Grading of monosodium iodoacetate-induced osteoarthritis reveals a concentration-dependent sensitization of nociceptors in the knee joint of the rat. Neurosci. Lett. 465 (2), 184-188 (2009).
- Vonsy, J. L., Ghandehari, J., Dickenson, A. H. Differential analgesic effects of morphine and gabapentin on behavioural measures of pain and disability in a model of osteoarthritis pain in rats. Eur. J. Pain. 13 (8), 786-793 (2009).
- Im, H. J., et al. Alteration of sensory neurons and spinal response to an experimental osteoarthritis pain model. Arthritis Rheum. 62 (10), 2995-3005 (2010).
- Sabri, M. I., Ochs, S. Inhibition of glyceraldehyde-3-phosphate dehydrogenase in mammalian nerve by iodoacetic acid. J. Neurochem. 18 (8), 1509-1514 (1971).
- van der Kraan, P. M., Vitters, E. L., van de Putte, L. B., van den Berg, W. B. Development of osteoarthritic lesions in mice by ‘metabolic’ and ‘mechanical’ alterations in the knee joints. Am. J. Pathol. 135 (6), 1001-1014 (1989).
- Guingamp, C., et al. Mono-iodoacetate-induced experimental osteoarthritis: a dose-response study of loss of mobility, morphology, and biochemistry. Arthritis Rheum. 40 (9), 1670-1679 (1997).
- Janusz, M. J., et al. Moderation of iodoacetate-induced experimental osteoarthritis in rats by matrix metalloproteinase inhibitors. Osteoarthr. Cartil. 9 (8), 751-760 (2001).
- Marker, C. L., Pomonis, J. D. The monosodium iodoacetate model of osteoarthritis pain in the rat. Methods Mol. Biol. 851, 239-248 (2012).
- Chaplan, S. R., Bach, F. W., Pogrel, J. W., Chung, J. M., Yaksh, T. L. Quantitative assessment of tactile allodynia in the rat paw. J. Neurosci. Methods. 53 (1), 55-63 (1994).
- Dixon, W. J. Efficient analysis of experimental observations. Ann. Rev. Pharmacol. Toxicol. 20, 441-462 (1980).
- Ogbonna, A. C., Clark, A. K., Gentry, C., Hobbs, C., Malcangio, M. Pain-like behaviour and spinal changes in the monosodium iodoacetate model of osteoarthritis in C57Bl/6 mice. Eur. J. Pain. 17 (4), 514-526 (2013).
- Fernihough, J., Gentry, C., Malcangio, M., Fox, A., Rediske, J., Pellas, T., Kidd, B., Bevan, S., Winter, J. Pain related behaviour in two models of osteoarthritis in the rat. Pain. 112 (1-2), 83-93 (2004).
