A schematic of a fully instrumented heart in retrograde perfusion (Figure 1A) and in left ventricular working heart (Figure 1B). Typical aortic, left atrial and left ventricular pressure and volume tracings are shown in Figure 2A – D. The typical end diastolic pressure is approximately 3 – 5 mmHg in this model, and the peak systolic pressure is approximately 100 mmHg. Figure 2E demonstrates the change in left atrial tracing when the LA cannula is moved away from the atrial septum during placement and positioning of the cannula. In these experiments, aortic pressure was set at 90 mmHg, and LA pressure was set to 10 mmHg.
To test the effects of catecholamines, each physiologic parameter (derived primarily from the pressure-volume catheter and associated software) was compared to the immediately preceding baseline period. In the example shown, dopamine was infused at 15 μg/kg/min into the left atrial block. Although the end diastolic pressure is identical in the two conditions (given the fixed atrial pressure in this model), the left ventricular end diastolic volume decreases by 2.5%, and the left ventricular end systolic volume decreases by 4.9%, yielding an increased stroke volume (Figure 3A). Compared with placebo infusions, the left ventricular stroke work, identified as the area within the pressure-volume curve, increased by 32% during treatment with dopamine (Figure 3B, P < 0.001, t test, n = 10 per group). This was associated with a greater increase in myocardial oxygen consumption relative to placebo infusions (Figure 3C). In this way, the relative potency and energy costs of different cardiotonic medications and doses can be compared to one another independent of their effects on loading conditions.
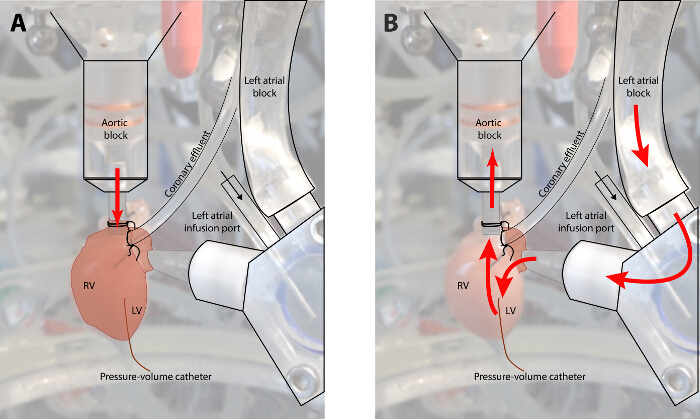
Figure 1: Diagram of Flow in a Fully Instrumented Heart in Retrograde Perfusion and Working Heart Mode. (Panel A: Langendorff mode; Panel B: working heart mode. In retrograde mode, KHB is infused at a set perfusion pressure into the aortic root. This mode is utilized to recover the myocardium following ischemic time and during instrumentation. In working heart mode, perfusate flows through the left heart before perfusing the coronary circulation. In this mode, the myocardium must generate its own perfusion pressure. Please click here to view a larger version of this figure.
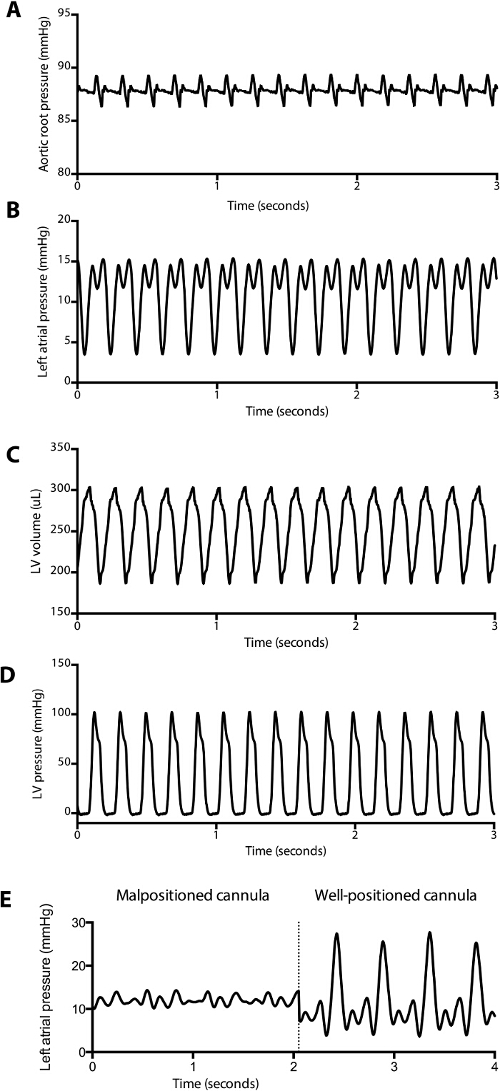
Figure 2: Representative Pressure and Volume Tracings Obtained during Baseline Measurements. (A) Aortic root pressure, (B) left atrial pressure, (C) left ventricular pressure and (D) left ventricular volume tracings during a baseline measurement are displayed. Stroke volume, stroke work, cardiac output, tau, and other parameters can be automatically calculated and displayed in real-time by the software. A blunted left atrial tracing (E) associated with a poor cardiac output in working heart mode can be a clue that the cannula is malpositioned in the left atrium. Note that the prominent v wave in the well-placed left atrial pressure tracing is common, likely due to a decreased left atrial compliance in the fully instrumented animal. Please click here to view a larger version of this figure.
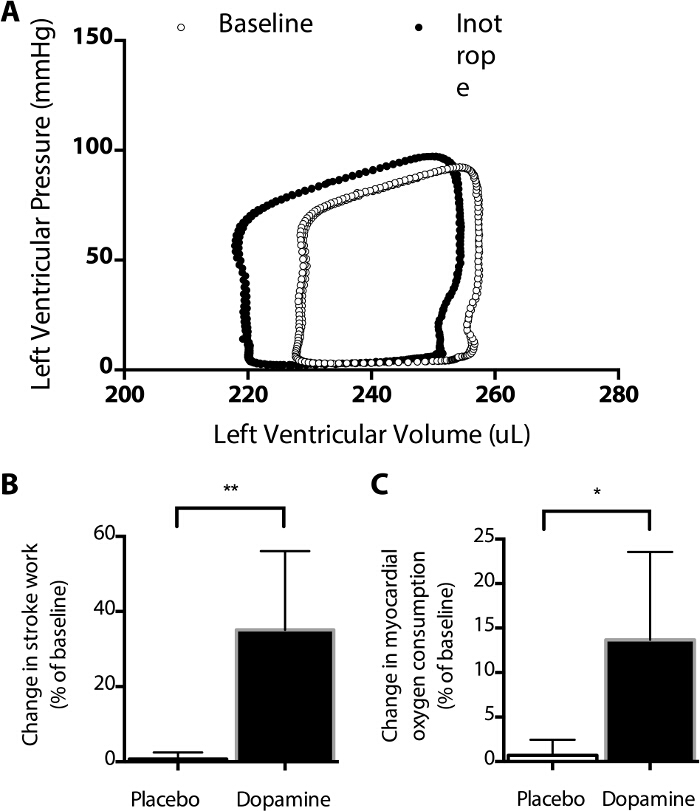
Figure 3: Effect of Dopamine on the Pressure-Volume Curve. Dopamine infusion results in a leftward shift in the PV curve (A), including an increased stroke volume, decreased end systolic volume, compared with baseline measurements. Note that the shape of some components of these PV curves differ from those typically measured in vivo (see Figure 4) due to the absence of arterial and venous elastance. (B) Relative to an immediately preceding baseline, stroke work increased significantly more during infusions of dopamine than placebo (**, P = 0.0017, t-test), as did myocardial oxygen consumption (*, P = 0.013, t-test, C). Using this model, the average myocardial oxygen consumption at baseline was 0.22 ± 0.02 mmol O2/gram tissue/minute, using an estimated dissolved oxygen content of 165 µmol/L in saline at 40 °C. Such measurements can be used to compare the myocardial oxygen consumption of various medications. Please click here to view a larger version of this figure.
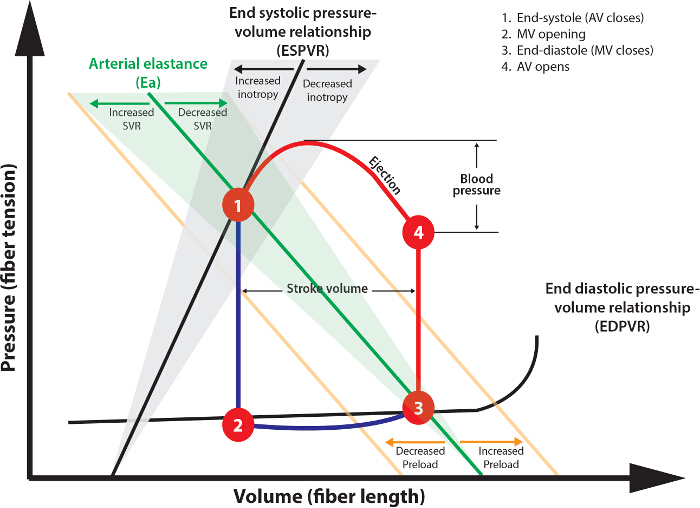
Figure 4: Analysis of Pressure Volume Loops. The Theoretical Pressure-Volume Loop Shown Describes the Normal Cardiac Cycle. Following aortic valve (AV) closure (1), isovolemic contraction occurs (1 – 2) as ventricular pressure decreases below atrial pressure. The duration of this phase is represented by Tau. The mitral valve (MV) then opens contemporaneously with atrial systole, filling the ventricle (2 – 3). Systole then commences with isovolemic contraction (3 – 4) until ventricular pressure exceeds diastolic arterial pressure, at which time the AV opens. Stroke volume is the difference between lines 1 – 2 and 3 – 4. Stroke work is the area within the 1 – 2 – 3 – 4 curve. Please click here to view a larger version of this figure.
