Location of the Parathyroid Glands
First, we recorded the distribution of the parathyroid glands of 54 PTHcre-mTmG mice as observed under the fluorescent dissection microscope. 74% (40/54) mice had two green parathyroid glands (Figure 1A, C, E), 26% (14/54) mice had an additional third parathyroid gland (Figure 1B, D, F). No mouse with a single gland or more than three glands were observed. Usually, parathyroid glands were located near the superior border of the thyroid gland (58%, 71/122; Figure 1A(1,2), B(1,2), C(2), D(1,2), E(2), F(3)). 27% (33/122) glands were located near the inferior border of the thyroid gland (Figure 1C(1), D(3), F(1)), and 13% (16/122) were located away from the thyroid gland (Figure 1B(3), E(1), F(2)). Our findings are consistent with and extend previous findings of varying locations of the parathyroid glands20.
GFP-PTX Mice
The entire surgery from anesthesia to closing the skin incision took approximately 20 min per mouse. The survival rate of postsurgical mice over a 3-month observation period was 96.3% (53/55). 92.4% (49/53) GFP-PTX mice exhibited ionized calcium levels that were 2 SD below the mean of sham-operated control mice or lower. The hypoparathyroid phenotype in the GFP-PTX mice (hypocalcemia, low PTH and elevated serum phosphate) was stable for the entire observation time of 3 months. Importantly, thyroid function was not different from sham-operated animals 3 months after surgery (TSH = 42 ± 24 vs. 30 ± 15 mU/L, p = 0.171; T4 = 3.0 ± 0.6 vs. 3.1 ± 0.9 µg/dL, p = 0.707 (Figure 2).
PTH-cre-iDTR Mice
DT injected PTH-Cre-iDTR mice developed hypoparathyroidism (low blood ionized calcium, elevated blood phosphorus, and inappropriately low-normal PTH levels). We have previously reported that a few PTH positive cells escape the ablation by diphtheria toxin, explaining the measurable circulating PTH and the therefore the somewhat milder phenotype of these mice17.
Hypoparathyroidism in GFP-PTX Mice and PTH-cre-iDTR Mice
Significant reductions of blood Ca++ and serum PTH levels were observed in GFP-PTX mice 3 days after surgery, compared to levels found in sham-operated mice (Ca++ = 1.05 ± 0.40 vs. 1.30 ± 0.03 mmol/L, p < 0.05; PTH=32 ± 22 vs. 580 ± 137 pg/mL, p < 0.05). The hypoparathyroidism phenotype was stable over the 3-month observation period (Figure 3A, reprinted with permission from (reference#17)). After 2 injections of 5 µg/kg DT at 3 days interval, a dose and regimen optimized to use the least amount of DT to give the maximal hypoparathyroid phenotype, the DT injected PTH-cre-iDTR mice showed significant hypocalcemia and reduced PTH compared to vehicle control mice, which persisted over the 90 days observation period (Ca++ = 1.10 ± 0.07 mmol/L vs. 1.26 ± 0.05 mmol/L, p < 0.05; PTH = 218 ± 156 pg/mL vs. 572 ± 164 pg/mL, p < 0.05) (Figure 3B, reprinted with permission from (reference#17)).
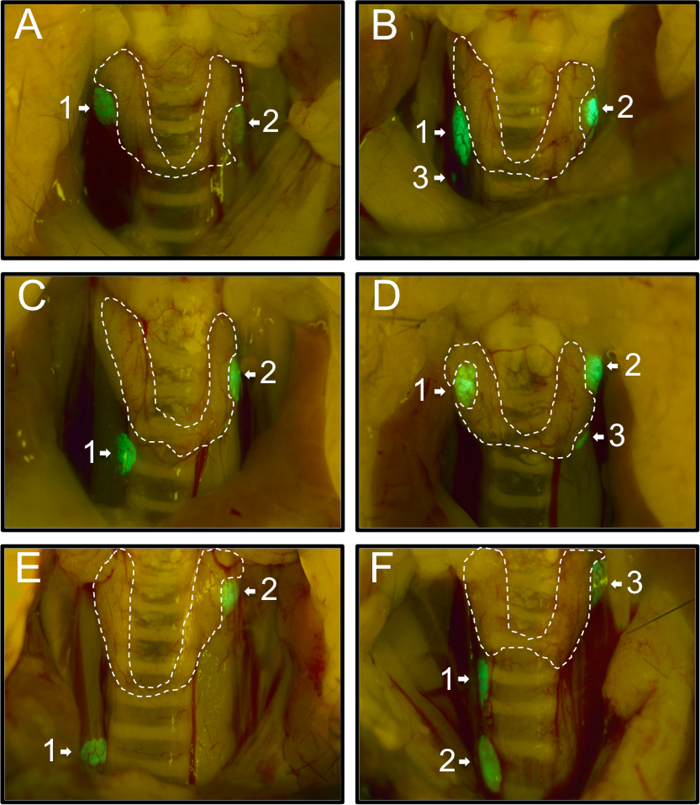
Figure 1: Representative Images of the Various Locations of the Parathyroid Glands in 54 PTHcre-mTmG Mice under Fluorescent Dissection Microscope. Mice had either two (A, C, E) or three (B, D, F) green parathyroid glands. Most parathyroid glands were located near the superior border (A(1,2), B(1,2), C(2), D(1,2), E(2), F(3) or near the inferior border of the thyroid gland (C(1), D(3), F(1)). In rare cases, some were located ectopically (B(3), E(1), F(2)). Please click here to view a larger version of this figure.
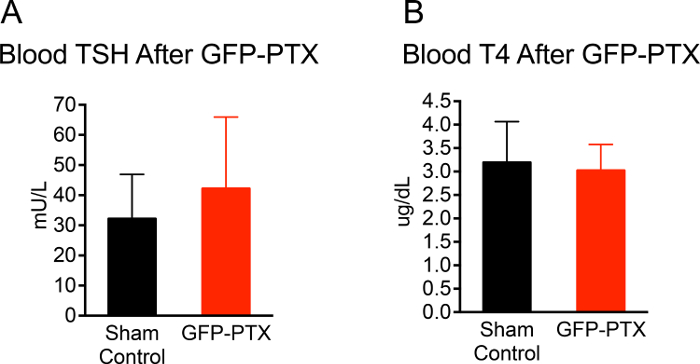
Figure 2: TSH and T4 Level of GFP-PTX Mice. 3 months after GFP-PTX, serum was obtained for TSH and T4 measurements. GFP-PTX mice showed TSH concentrations (42 ± 24 mU/L) (A) and T4 concentrations (3.0 ± 0.6 μg/dL) (B) that were not different from control mice (TSH = 30 ± 15 mU/L, p = 0.171, n =11, T4 = 3.1 ± 0.9, p = 0.707, n = 11). Please click here to view a larger version of this figure.
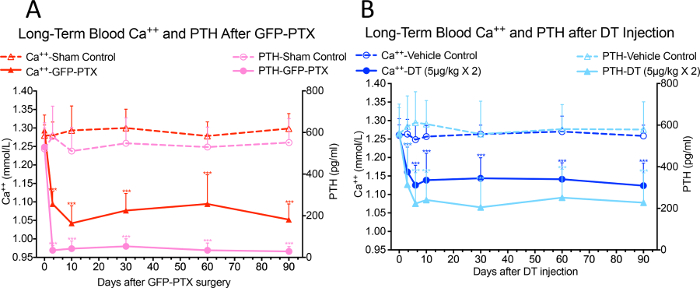
Figure 3: Blood Ca++ and PTH Levels in GFP-PTX Mice and DT Injected PTH-cre-iDTR Mice. Both GFP-PTX mice (A) and DT injected PTH-cre-iDTR mice (B) exhibited stable hypocalcemia and reduced PTH levels over 3 month observation period (N = 6 – 8, ***p < 0.001) (re-printed with permission from reference#17). Please click here to view a larger version of this figure.
