All animal studies were carried out in accordance with the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health with approval from the Institutional Animal Care and Use Committee of the NIAID (NIH), Bethesda, MD. All studies involving M. tuberculosis were performed in a laboratory with biosafety containment level 3 (BSL-3).
1. Rabbit Infection Model and Caseum Collection
- Infect New Zealand white rabbits with M. tuberculosis using a nose-only aerosol exposure system as previously described.12,13 Allow the infection to progress for 12-16 weeks. Sedate the rabbits with 35 mg/kg ketamine and 5 mg/kg xylazine intramuscularly, euthanize the rabbits with 0.22 mL/kg pentobarbital sodium and phenytoin sodium intravenously and proceed with the necropsies.
- Using tweezers and a scalpel, remove lungs from the chest cavity. From each lung lobe, dissect out individual cavities and large necrotic granulomas using a scalpel. Carefully scrape off caseum from the cavity and granuloma walls. Weigh, record and store samples in 2 mL screw-capped tubes at -20 °C until ready for use.
- Gamma-irradiate the infectious caseum samples at 3 MegaRad on dry ice to render them uninfectious and safe for use in a BSL-2 lab.
2. In Vitro Generation of Caseum Surrogate from THP-1 Cells
- Grow THP-1 monocytes in RPMI 1640 medium (2 mM L-glutamine and 10% fetal bovine serum) in T175 cell culture flasks (80 mL/flask). Incubate the flasks in a 5% CO2 atmosphere at 37 °C for 3-4 days.
- Centrifuge the culture from a T175 flask in two 50 mL conical tubes at 150 x g for 5 min. Discard the supernatant and suspend the pellet in 10 mL of RPMI 1640 media.
- Pipette 5 µL of this culture into a 1.5 mL tube containing 45 µL of trypan blue. Mix thoroughly by pipetting. Transfer 10 µL to a hemocytometer and count the number of viable THP-1 monocytes (unstained) using a light microscope (10X magnification). Calculate the number of viable cells per mL of the culture. Dilute it with RPMI media to the final density of 1.25 x 106 cells/mL.
- Load 40 mL of the culture on a large cell culture plate (50 x 106 cells/plate). Add 40 µL of 100 µM PMA (phorbol 12-myristate13-acetate prepared in ethanol) and allow cells to adhere overnight in the incubator.
NOTE: Final concentration of PMA is 100 nM. - Dilute pure oleic acid (OA) (0.89 g/mL) in ethanol to the concentration of 0.1 M (i.e. 31.7 µL OA in 968.3 µL ethanol). Dilute this solution in fresh pre-warmed RMPI media to a concentration of 10 mM. Dilute this OA suspension to 0.4 mM (final working concentration) in RPMI medium pre-warmed to 37 °C.
- Remove the existing media and non-adhered cells from the cell culture plates and gently add 40 mL of 0.4 mM OA to the THP-1 macrophages (THP-M). Incubate at 37 °C in the incubator overnight.
- Use a light microscope at 40x magnification to visually confirm the presence of numerous lipid body inclusions in each THP-M. Remove all RPMI medium from the cell culture plates and gently wash the adherent cells twice with phosphate buffered saline (PBS) using a 50 mL serological pipette.
NOTE: Lipid bodies appear as small, clear, spherical structures in the cytoplasm of the THP-M. - Add 40 mL of 5 mM ethylenediaminetetraacetic acid (EDTA) in PBS to each plate. Incubate for 15 min at 37 °C.
- Detach the foamy macrophages (FM) by repeatedly pipetting up and down over the surface of the whole plate using a 10-mL serological pipette. Transfer the cell suspension to a 50-mL conical tube and spin down at 150 x g for 5 min.
- Resuspend the cell pellet in 10 mL of PBS (third PBS wash) and transfer to a pre-weighed 15-mL conical tubes. Spin down again at 150 x g for 5 min. Carefully aspirate the supernatant using a serological pipette and discard.
- Subject the FM pellets to 3 freeze-thaw cycles to lyse the cells and incubate them at 75 °C for 20-30 min to denature proteins in the matrix. Store the pellets at -20 °C until ready for use.
3. Rapid Equilibration Dialysis (RED) Assay
- Prepare 10 mM stock solutions of all test compounds in dimethyl sulfoxide (DMSO). Dilute to 500 µM working solutions in DMSO prior to each assay.
- Weigh the tube containing the caseum surrogate pellet. Subtract the weight of the empty tube to derive the weight of the pellet alone. Add 2-3 metal beads per tube and, using a tissue homogenizer at 1,200 strokes/min for 1 min, disrupt caseum or the surrogate matrix in PBS (1:9 w/v) to achieve 10x diluted suspension of each matrix.
- Spike 6.5 µL of the 500 µM solution of the test compound into 643.5 µL of the homogenate to achieve the final concentration of 5 µM (≤1% DMSO) and vortex.
- Place the RED inserts into the base plate. Add 200 µL of the drug-spiked matrix into the donor chamber (red ring) of each RED insert and 350 µL of PBS into each receiver chamber. Prepare 3 inserts for each test compound (triplicate samples). Seal plate with an adhesive plate seal and incubate at 37 °C on the thermomixer at 200 rpm (1 x g) for 4 h.
- After the incubation, gently mix the contents of the donor and receiver chambers by pipetting up and down 2-3 times. Pipette out 20 µL aliquots of homogenate from the donor chambers and add to 20 µL of clean PBS in a 1.5 mL tube (1:1). Similarly, pipette out 20 µL aliquots of PBS samples from the receiver chambers and add to 20 µL of clean homogenate (matrix matching).8
NOTE: Matrix-matching eliminates the need for 2 separate calibration curves (in homogenate and PBS) to be made for quantitative analysis. Contents of the donor chamber may sediment over time. Gently mix the contents by pipetting prior to removing aliquots.
4. LC-MS Quantification and Data Analysis
- Add 160 µL of 1:1 methanol:acetonitrile containing 500 ng/mL diclofenac or 10 ng/mL verapamil (internal standard) to each tube and vortex to precipitate proteins. Centrifuge at 10,000 x g for 5 min to sediment the precipitate and transfer supernatants into 96-well deep-well plates for liquid chromatography-mass spectrometry (LCMS) analysis.7
- Build calibration curves from 1-1,000 nM for each test compound while keeping the same matrix composition as the samples above. Quantify the concentration of test compound in samples from the donor and receiver chambers using an LC-MS method.
- Calculate the unbound fraction (fu) of the drug in diluted matrix using equation 1. Calculate the fu in undiluted matrix using equation 2 (D = dilution factor of 10).14
- Check the recovery (mass balance) of each compound using equation 3 to identify compounds with stability/metabolism/non-specific binding issues.
NOTE: Recovery typically falls between 70% and 130%.15

Using this protocol, we have tested hundreds of tuberculosis drug development compounds for their predicted efficiency at penetrating caseum. Figure 1 visualizes the basic concepts of the RED assay. The dialysis membrane of the RED inserts allows for unbound small molecules to diffuse from the donor well to the receiver well, finally achieving an equilibrium between both compartments. Small molecules that are bound to macromolecules such as proteins or lipids are trapped in the donor well. Quantitative analysis of the samples from both compartments allows for the calculation of the unbound fraction (fu) of each small molecule in the caseum or surrogate matrix. This fraction has been shown to directly correlate with drug penetration in caseum in vivo.7 As Figure 2 illustrates using MALDI (Matrix-assisted laser desorption/ionization) mass spectrometry images, the higher the fu, the more extensively the drug diffuses into caseum. Hence, this agrees with the hypothesis that as drug molecules diffuse into the outer rim of caseum from its interface with cellular layers of the lesion, binding to caseous macromolecules sequesters the drug, preventing it from further diffusing into the caseous core. A sample panel of 18 anti-tuberculosis drugs is listed in Table 1 along with their fu in both caseum and the surrogate. As Figure 3 illustrates, the matrix prepared from THP-1-derived foamy macrophages is an effective surrogate to true caseum. Binding in both matrices strongly correlates with each other.
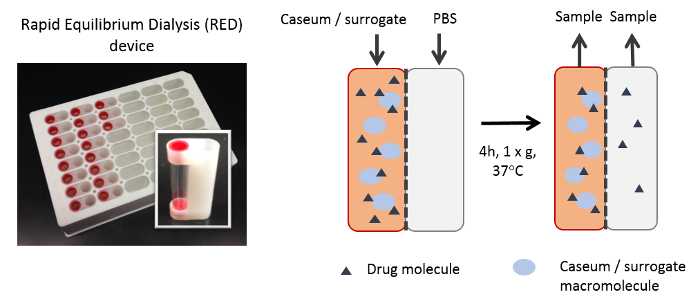
Figure 1: Illustration of the RED assay. During incubation, drug molecules that remain unbound to macromolecules in the matrix diffuse across the dialysis membrane. Over time, an equilibrium is established between the concentration of unbound drug molecules in both the donor and receiver wells. All macromolecules (proteins, lipids, etc.) and bound drug molecules are trapped within the donor chamber. Please click here to view a larger version of this figure.
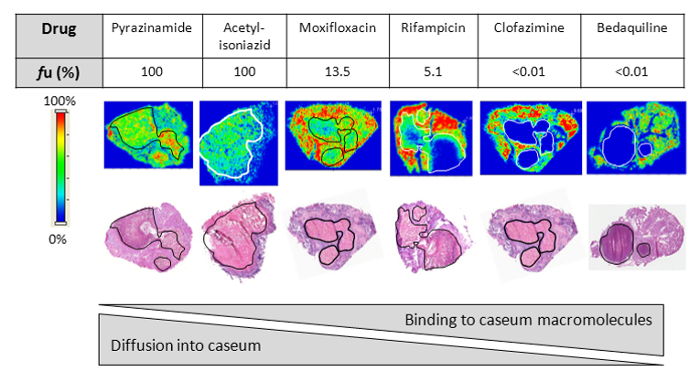
Figure 2: Drug penetration in vivo. Relationship between the fraction unbound (fu) and diffusion into caseum in vivo as determined by MALDI (matrix-assisted laser desorption/ionization) mass spectrometry imaging for six anti-tuberculosis drugs. Ion maps are of representative lung lesions and the signal intensity is indicated by the scale bar to the left. Hematoxylin and Eosin (H&E) staining of adjacent sections is shown below the ion maps. Black/white contour lines highlight the caseous center of each lesion. Reprinted (adapted) with permission from Sarathy et al.7 Please click here to view a larger version of this figure.
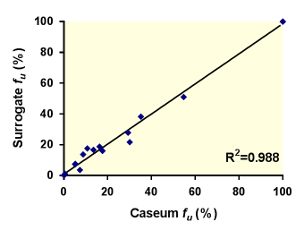
Figure 3: Correlation between the unbound fractions (fu) of 18 anti-tuberculosis drugs in caseum and the surrogate matrix. The best-fit line was determined using linear regression. The goodness of fit is expressed as the R2 value. Reprinted (adapted) with permission from Sarathy et al.7 Please click here to view a larger version of this figure.
| Caseum fu (%) | Surrogate fu (%) | |
| Ethambutol | 35.2 ± 4.4 | 38.8 ± 5.6 |
| Isoniazid | >99.9 | >99.9 |
| Acetyl-isoniazid | >99.9 | >99.9 |
| p-aminosalicylic acid | 54.7 ± 1.4 | 51.1 ± 11.2 |
| Rifampicin | 5.13 ± 0.2 | 7.3 ± 0.6 |
| Rifapentine | 0.5 ± 0.1 | 1.1 ± 0.1 |
| Moxifloxacin | 13.5 ± 3.7 | 16.8 ± 1.8 |
| Levofloxacin | 8.34 ± 0.4 | 16.3 ± 3.1 |
| Gatifloxacin | 16.3 ± 4.2 | 18.8 ± 2.9 |
| Linezolid | 29.3 ± 3.6 | 27.9 ± 2.2 |
| Posizolid | 10.7 ± 1.7 | 17.6 ± 4.5 |
| Sutezolid | 30.1 ± 8.7 | 21.7 ± 1.7 |
| Radezolid | 5.2 ± 0.8 | 7.6 ± 1.9 |
| Tedizolid | 8.8 ± 1.8 | 13.7 ± 2.7 |
| Clofazimine | <0.01 | <0.01 |
| Bedaquiline | <0.01 | <0.01 |
| PA-824 | 7.31 ± 2.2 | 3.6 ± 0.2 |
| OPC67683 | 0.04 ± 0.02 | 0.02 ± 0.002 |
Table 1: Fraction unbound (fu) of the 18 TB drugs tested in the caseum and surrogate binding assay. All results are expressed as the mean ± standard deviation. Reprinted (adapted) with permission from Sarathy et al.7
