The surgical procedures described above allow the production of a consistent and reproducible lateral HX at T9. After perfusion and skin removal, the surgical site at T9 could be readily identified by a residual suture (Figure 6A). Further dissection allows the exposure of the cement bridge (Figure 6B), and gelatin sponge (Figure 6C) in layers. The spinal cord is then exposed to the opened vertebral canal and a lateral hemisection on the right side is confirmed (Figure 4D). The level of the injury can be further confirmed by its association with the exposed vertebral bodies and ribs (Figure 6D). Immunofluorescence staining of a cross-section at the injury epicenter shows a complete loss of right hemicord and the preservation of the left hemicord contralateral to the injury. The section stained with an axon marker SMI-31 and astrocytic marker glial fibrillary acidic protein (GFAP) (Figure 6E).
Neurobehaviorally, the CBS-HX system is capable of detecting asymmetric deficits over time following a T9 HX. After HX, the ipsilateral hindlimb lost its ability to step whereas the contralateral hindlimb retained the ability to walk. For each behavior measure, we performed 3 trials and used the mean of the 3 trials for quantification and analysis. We used pre-surgery measure as a baseline which we consider as the most accurate control as compared with using other rats. Scores of the 4 individual measures, i.e. UHS, CPL, contact placing, and grid walking can be analyzed separately (Figure 7A-D) or they can be combined into a composite CBS-HX (Figure 7E). Two-way ANOVA analyses showed significant differences in UHS (F = 23.199, p < 0.001), coupling (F = 8.376, p < 0.01), contact placing (F = 17.672, p < 0.001), grid walking (F = 19.261, p < 0.001), CBS-HX (F = 20.897, p < 0.001) between the ipsilateral and contralateral sides. Figure 7A shows the results of UHS after a T9 HX. In the first 3 days postinjury, rats lost the ability to step and received a score of 0-2 for the ipsilesional hindlimb. Step-like movements began to appear on the ipsilesional side at 7-10 days after injury with most steps being dorsal steps. By 28 days after the T9 HX, the rats could take plantar steps with virtually normal coordination with an assigned UHS score of 8. As a comparison, the contralesional hindlimb was less interrupted and the UHS score dropped within the first 5 days after the T9 HX and returned to the baseline level after day 10 post-injury. For the total CPL (including homolateral, homologous and diagonal coupling) test, both stability and adaptability of coordination after T9 HX were markedly reduced (Figure 7B). At 1-5 days after injury, the HX animals showed no sign of CPL. Over time, CPL of the ipsilateral hindlimb emerged, often clumsy, unsteady, and inappropriately varying in their speed, force, and direction. The contact placing (Figure 7C) and grid walking (Figure 7D) of the ipsilateral hindlimb were also affected by the T9 HX particularly within the first 5 days after the injury, and usually recovered when the animal began to take plantar steps. The composite CBS-HX system includes the UHS, CPL, contact placing, and grid walking tests for a maximum possible score of 18 (Figure 7E). The motor function of the ipsilateral hindlimbs demonstrated a decrease in CBS-HX scores after the T9 lateral HX, which is consistent with the deficits seen in the human Brown-Séquard syndrome. The motor function of the ipsilateral hindlimbs demonstrated a decrease in CBS-HX scores from 1 day to 4 weeks after the T9 lateral HX as compared to the contralateral hindlimbs (Figure 7E).
Thus, the composite CBS-HX system combining the UHS, CPL, contact placing, and grid walking can be used to evaluate the behavioral function of rats after the lateral injury of the thoracic spinal cord for a maximum possible score of 18.
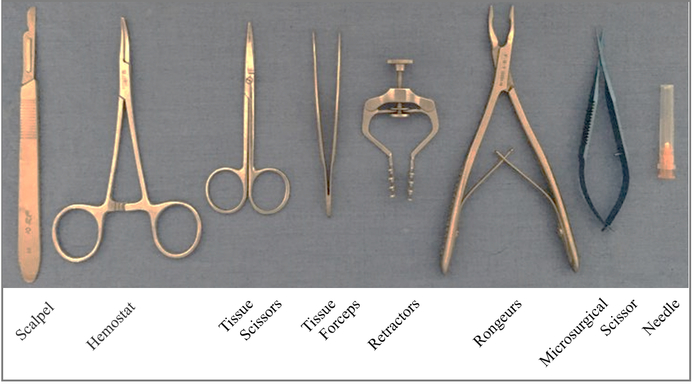
Figure 1. Surgical tools used for producing a T9 right-sided hemisection. Please click here to view a larger version of this figure.
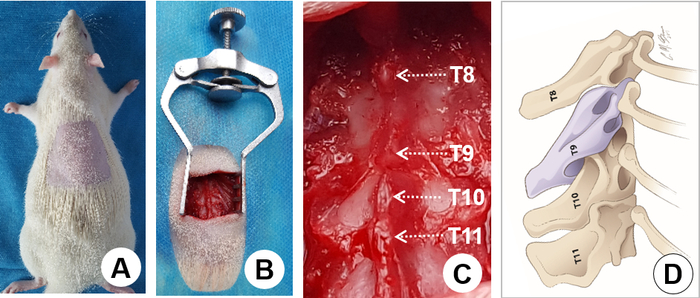
Figure 2. Surgical exposure. A) Shave the hair on the back overlying the surgical region. B) Retract muscles from the surgical area using a retractor. C) Expose the T8-11 vertebral laminae and define individual spinous processes (arrows). Note that there is a large gap between the T8 and T9 spinous processes, which is a landmark for identifying T9. D) The schematic drawing shows the lateral view of the spinous processes. The T9-11 spinous processes form a pyramid with the T10 spinous process being the peak. Again, a large gap between the T8 and T9 spinous processes is clearly seen as a landmark for identifying T9 where a laminectomy is performed. Please click here to view a larger version of this figure.
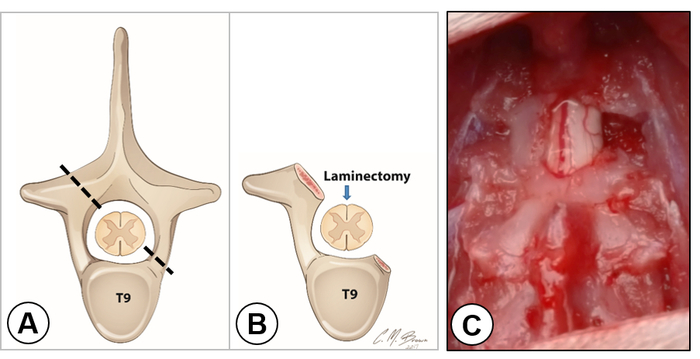
Figure 3. Laminectomy and exposure of the right hemicord. A) The schematic drawing shows the cross section of the spinal cord within the T9 vertebra. The dashed line indicates the extent of laminectomy on each side. B) The schematic drawing shows the removal of a small portion of the lamina on the left side and the entire vertebral arch on the right side. An arrow indicates the dorsal midline of the cord. C) Dorsal view of the exposed spinal cord. Note that the dorsal vein was located in the middle of the spinal cord dividing the left and right hemicords. The right hemicord was completely exposed. Please click here to view a larger version of this figure.
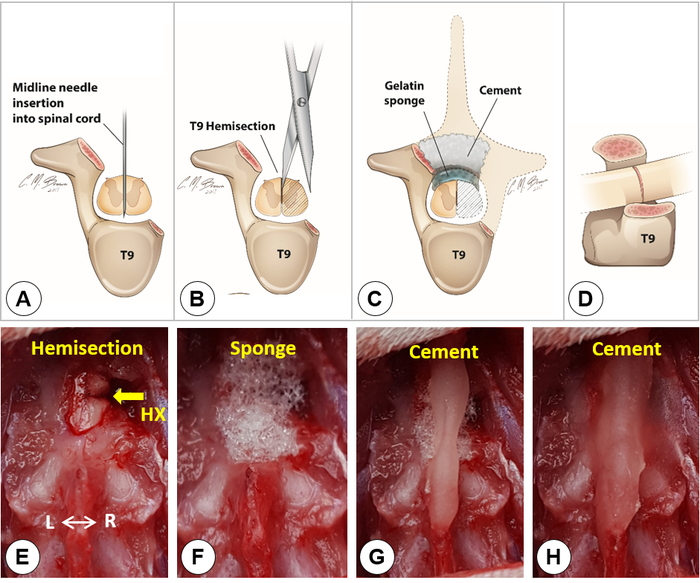
Figure 4. Lateral hemisection. A-D) Schematic drawings show the midline needle insertion into the spinal cord (A), the T9 hemisection (B), the covering of gelatin sponge and cement (C), and the lateral view of a T9 lateral hemisection (D). Dashed lines in C outline the removed T9 vertebral lamina and the right hemicord. E) Dorsal view of a right spinal cord hemisection. F) Placement of a small piece of gelatin sponge over the hemisection site. G-H) A Simplex-P cement bridge built over the sponge and the spinous processes of T8 and T10. Please click here to view a larger version of this figure.
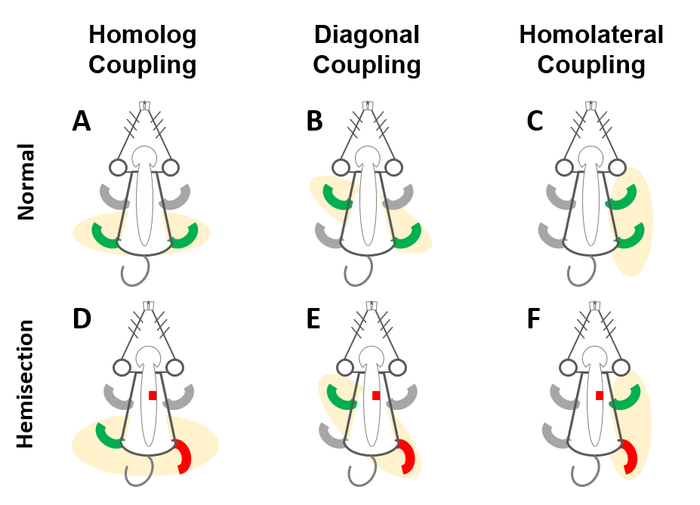
Figure 5. Schematic drawing of the coupling (CPL) test. The CPL test is to evaluate the coordination of alternating movements of limbs, including A) homologous CPL (front-front/rear-rear limbs), B) diagonal CPL (front left-rear right/front right-rear left limbs), and C) homolateral CPL (front-rear limbs on the same side). After T9 HX (red box, D-F), the hindlimb deficit became visible on the ipsilesional side and animals show lack of coordination in homolog (D), diagonal (E), and homolateral (F) CPL. Please click here to view a larger version of this figure.
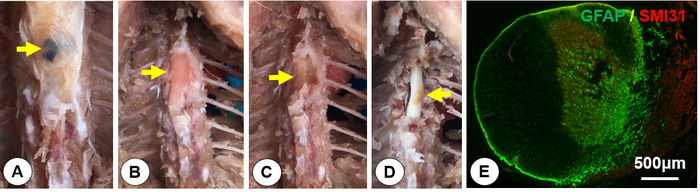
Figure 6. Tissue dissection and histology. After perfusion, tissues were dissected out to expose the spinal cord. Cross sections were processed for double immunofluorescent staining of glial fibrillary acidic protein (GFAP, a marker for astrocytes) and SMI31 (a marker for axons). A) Exposure of the suture as a landmark for the injury site (yellow arrow). B) Exposure of the dental cement (yellow arrow). C) Exposure of the gelatin sponge (yellow arrow). D) Identify the spinal hemisection on the right side (yellow arrow). E) A spinal cord cross section at the injury epicenter immunostained with GFAP (green) and SMI 31 (red). It shows that the right spinal hemicord was completely cut and the left hemicord was well preserved. Please click here to view a larger version of this figure.
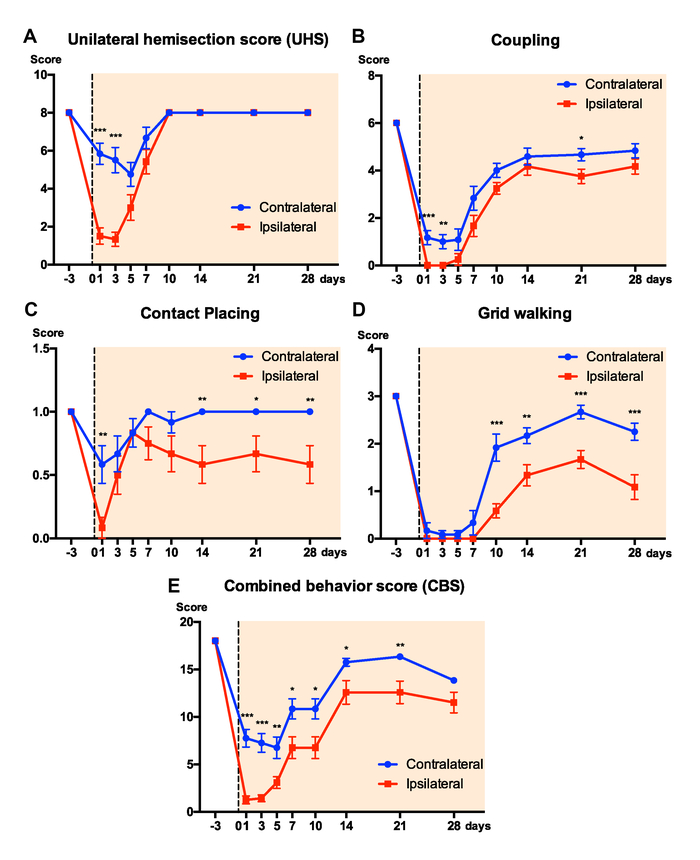
Figure 7. Results of neurobehavioral scores. Graphs show scores of the 5 measures: A, the unilateral hemisection score (UHS); B, coupling (CPL); C, contact placing; D, grid walking, and E, combined behavior score (CBS) on ipsilateral and contralateral hindlimbs after a T9 HX. Data represent mean ± s.e.m. *: p < 0.05, **: p < 0.01, ***: p < 0.001 between ipsilateral and contralateral hindlimbs (Two-way ANOVA, Tukey's multiple comparisons test, n = 12 rats/groups). Please click here to view a larger version of this figure.
| Subscore Name/Range | Description | Score | |
| Unilateral hindlimb stepping | Observable slight hindlimb movement | No | 0 |
| (UHS) | Yes | 1 | |
| (0-8) | Movement of Ankle | No | 0 |
| Yes | 1 | ||
| Movement of Knee | No | 0 | |
| Yes | 1 | ||
| Movement of Hip | No | 0 | |
| Yes | 1 | ||
| Sweeping (no weight support) | No | 0 | |
| Yes | 1 | ||
| Placing (no weight support) | No | 0 | |
| Yes | 1 | ||
| Placing (with weight support) | No | 0 | |
| Yes | 1 | ||
| Stepping | No | 0 | |
| Yes | 1 | ||
| Coupling | Homolateral | No | 0 |
| (0-6) | Irregular/clumsy | 1 | |
| Normal | 2 | ||
| Homologous | No | 0 | |
| Irregular/clumsy | 1 | ||
| Normal | 2 | ||
| Diagonal | No | 0 | |
| Irregular/clumsy | 1 | ||
| Normal | 2 | ||
| Contact placing | No | 0 | |
| (0-1) | Yes | 1 | |
| Grid walking | Miss steps | >15 | 0 |
| (0-3) | ≤15 | 1 | |
| ≤10 | 2 | ||
| ≤5 | 3 | ||
| Total CBS-HX | |||
| (0-18) | |||
Table 1: The combined behavior scores for hemisection (CBS-HX)
