A total of 35 patients who underwent PVRP were included in one of our studies. The mean patient age was 72.1 ± 7.1 years (range 53-85 years).
Perioperative data are listed in Table 1. The mean laser emission time accounted for nearly 50% of the mean operative time. The blood loss in most patients was < 200 mL. However, the average deviated due to some moderate bleeding cases. Almost 90% of the patients had the catheter removed within 6 days postoperatively.
All patients returned to the hospital for follow-up examinations at the 1st and the 3rd month postoperatively (Table 2). Examinations including urinalysis combined with urine culture were performed to check for postoperative urinary tract infection (UTI).
International Prostate Symptom Score (IPSS) and Quality of Life (QoL) are tools used to screen for, rapidly diagnose, track the symptoms of, and suggest management of the symptoms of BPH. It also can be used to evaluate the efficacy of BPH treatment. Compared to baseline values, the mean subgroup IPSS and QoL scores improved dramatically during follow-up. The IPSS storage score, IPSS voiding score, IPSS nocturia score, and the QoL score significantly decreased by 75.3%, 83.6%, 51.4%, and 71.7%, respectively (all P < 0.001). For the objective parameters, the mean prostate volume and the serum level of the total prostatespecific antigen decreased to 42.6% and 36.2%, respectively. The mean Qmax increased nearly 2-fold compared to the baseline and reached a maximum of 15.6 mL/s. The mean postvoid residual during followup was only 11.9 ± 6.5 mL. Table 3 presents the peri and postoperative complications. According to the modified ClavienDindo classification system15 a widely used and authoritative tool for grading surgical complications, only two cases were Grade 3B, one was a prostate capsule perforation and the other was a bladder neck contracture. Prostate capsule perforation was identified in a single case, which did not require specific therapy. No other perioperative complications were found. Three patients experienced high febrility due to acute UTI caused by extendedspectrum betalactamase Escherichia coli on postoperative days 5-6; all three patients received antibiotics and recovered rapidly. Five patients complained of urgency and frequency, but the urine culture revealed no abnormalities in three of them which could exclude UTI. The other two patients were diagnosed with UTI according to urine culture and recovered after effective antibiotic courses. Only a single patient experienced persistent urinary incontinence in the early postoperative period without evidence of UTI. This urinary incontinence was fully resolved after pelvic floor muscles training for several weeks. Another patient with difficulty in voiding was diagnosed with bladder neck contracture through cystoscopy. This was resolved after a bladder neck incision was performed under general anesthesia on the 40th day after PVRP.
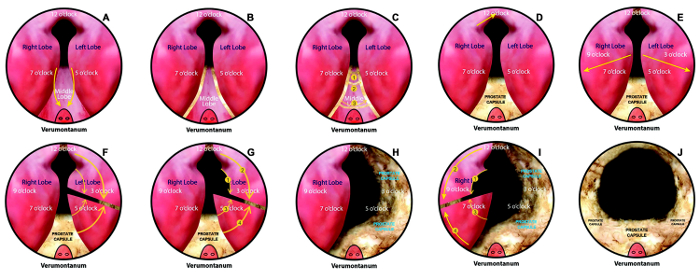
Figure 1: Key steps of photoselective vaporesection of the prostate. (A) Mark two lines originally at 5 o'clock and 7 o'clock at the bladder neck. These lines continue along the boundaries between the median and lateral lobes. (B, C) Vaporize the prostate tissue via laser vaporization along these lines, they are merged into single line adjacent to the verumontanum. Mark several lines on the surface of the middle lobe via laser fiber, divide the middle lobe into several chunks through vaporization technique and then split each chunk from the middle lobe, finally remove the whole middle lobe. (D) Vaporize the tissue at 12 o'clock from the apex of the prostate to the bladder neck. (E) Set another two similar grooves that originated from the bladder neck at 3 o'clock and 9 o'clock to the proximal end of the verumontanum. (F-I) Remove the tissue of the lateral glands, the technique is similar to middle lobe resection. (J) Channel trimming. Please click here to view a larger version of this figure.
| Perioperative data of 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate |
||||
| Data are shown as mean ± SD, or otherwise noted. TURP: Transurethral resection of the prostate; BPH: Benign prostatic hyperplasia; SD: Standard deviation. | ||||
| Parameters | Data | |||
| Mean operative time (min) | 119.4 ± 41.1 | |||
| Mean laser time (min) | 58.9 ± 22.3 | |||
| Blood loss (ml) | 204.6 ± 129.4 | |||
| Bladder irrigation during the operation (L) | 40.4 ± 14.2 | |||
| Convert into TURP (n) | 4 | |||
| Postoperative pathology report, n | ||||
| BPH | 33 | |||
| Prostate cancer | 2 | |||
| Catheterization time (days) | 7.4 ± 2.0 | |||
| Postoperative hospital stay (days) | 7.3 ± 1.4 | |||
Table 1: Perioperative data of 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate. Data are shown as mean ± SD or otherwise noted. TURP: Transurethral resection of the prostate; BPH: Benign prostatic hyperplasia; SD: Standard deviation.
| Pre- and post-operative functional parameters of 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate | |||||
| Data are shown as mean ± SD. *Significant differences between pre- and post-operative 1 month groups; †Significant differences between pre- and post-operative 3 months groups; ‡Significant differences between postoperative 1 month and postoperative 3 months groups. IPSS: International Prostate Symptom Score; QoL: Quality of life; Qmax: Maximal urinary flow rate; tPSA: Total prostate-specific antigen; SD: Standard deviation. |
|||||
| Parameters | Preoperative (n = 35) | Postoperative 1 month (n = 35) | Postoperative 3 months (n = 35) | F | P |
| Storage scores in IPSS | 8.9 ± 3.3*,† | 4.4 ± 3.6‡ | 2.2 ± 1.9 | 33.025 | <0.001 |
| Voiding score in IPSS | 11.0 ± 3.2*,† | 4.1 ± 3.9‡ | 1.8 ± 1.7 | 86.58 | <0.001 |
| Nocturia score in PSS | 3.7 ± 1.1*,† | 2.4 ± 1.1‡ | 1.8 ± 0.9 | 29.15 | <0.001 |
| QoL score | 4.6 ± 0.9*,† | 2.3 ± 1.5‡ | 1.3 ± 1.0 | 107.08 | <0.001 |
| Prostate volume | 81.1 ± 36.6*,† | 35.4 ± 14.2‡ | 34.0 ± 14.1 | 45.83 | <0.001 |
| Qmax | 5.3 ± 3.9*,† | 12.5 ± 3.4‡ | 16.0 ± 4.3 | 58.84 | <0.001 |
| tPSA | 5.8 ± 4.6*,† | 3.1 ± 2.8‡ | 2.1 ± 1.7 | 12.21 | <0.001 |
Table 2: Pre– and post–operative functional parameters of 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate. Data are shown as mean ± SD. *Significant differences between pre- and post-operative 1-month groups; †Significant differences between pre- and post-operative 3-months groups; ‡Significant differences between postoperative 1-month and postoperative 3-months groups. IPSS: International Prostate Symptom Score; QoL: Quality of life; Qmax: Maximal urinary flow rate; tPSA: Total prostate-specific antigen; SD: Standard deviation.
| Peri- and post-operative complications in 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate |
||
| Complications were graded according to the modified Clavien-Dindo classification system. TURP: Transurethral resection of the prostate. | ||
| Complications | Patients, n (%) | Grade |
| Intraoperative | ||
| Acute urinary tract infection | 3 (8.6) | 2 |
| Prostate capsule perforation | 1 (2.9) | 3b |
| Blood transfusion | 0 | 2 |
| TURP syndrome | 0 | 4 |
| Bladder wall injury | 0 | 2 |
| Ureteric orifice injury | 0 | 2 |
| Urethra sphincter injury | 0 | 2 |
| Postoperative | ||
| Urinary tract infection | 2 (5.7) | 2 |
| Urinary incontinence | 1 (2.9) | 1 |
| Bladder neck contracture | 1 (2.9) | 3b |
| Postoperative bleeding | 0 | 2 |
Table 3: Peri– and post–operative complications in 35 patients with benign prostatic hyperplasia who underwent photoselective vaporesection of the prostate. Complications were graded according to the modified Clavien-Dindo classification system. TURP: Transurethral resection of the prostate.
