The current protocol, describing the mini-endoscopic evaluation of intestinal GvHD-associated lesions of the distal colon, has been established and validated in mice previously subjected to the systemic induction of a severe acute GvHD model. In this study, we used an MHC class I fully mismatched model system in which BALB/c mice were lethally irradiated, followed by the transplantation of T-cell-depleted allogeneic bone marrow and by the administration of GvHD-inducing alloreactive C57BL/6 CD3+ T lymphocytes. T-cell-depleted bone marrow cells and splenic T cells for GvHD induction were purified by magnetic separation. The purity of these cell populations was determined by flow cytometry, and representative results of the purification process are displayed in Figure 1, showing a sufficient depletion of T cells from total bone marrow cells and a consistent enrichment of spleen-derived CD3+ T cells prior to their transfer to previously irradiated mice. The clinical course displayed in Figure 2 demonstrates the reproducibly robust induction of the clinical systemic GvHD phenotype upon allo-HCT in the presence (WT, in black) vs. absence (noT, grey) of alloreactive donor T lymphocytes. The scoring system previously reported by Cooke et al. represents a sum core in which six parameters are assessed and graded: body weight, posture, activity, skin and fur texture, and stool consistency6. The control mice experienced only one, early occurring peak of the clinical score, between days 5 and 10, that was similarly observed in T-cell-receiving mice and is, therefore, largely due to the irradiation-associated systemic inflammatory response. Regardless, clinical scores of donor T-cell-receiving mice started to rise earlier, showed a higher total peak, only transiently decreased after initially peaking, and then, essentially increased again, continuously, over the remaining period of the experiment. Overall, these results are in agreement with the interpretation that T-cell-receiving mice show stronger and more progressive signs of systemic GvHD compared to noT mice.
The donor T-lymphocytes-receiving allo-HCT mice showed various signs of acute organ-related and systemic GvHD manifestations, overall resulting in high sum scores, while the control mice lacked moderate to severe affections, especially at later time points. However, signs of intestinal GvHD are underrepresented in the systemic GvHD scoring system, where the only assessed gut-related parameter is stool consistency. As shown in Table 1, mini-endoscopically assessable criteria were defined, specifically intended for the precise description, scoring, and grading of intestinal GvHD-associated lesions, by adapting criteria previously reported for the evaluation of syngeneic colitis to the context of alloresponse-driven colitis9. Figure 3 displays typical examples for each individual criterion, illustrating the type and extent of intestinal GvHD-associated lesions, thereby visualizing the grading matrix applied during the mini-endoscopic evaluation of the distal colon of GvHD-prone mice upon transplantation of MHC class I fully mismatched donor lymphocytes.
Figure 4A shows that intestinal GvHD sum score results that are based on criteria defined in Table 1 and displayed in Figure 2 easily enable the experimenter to discriminate donor lymphocyte-receiving mice with severe signs of intestinal inflammation from control mice that are essentially devoid of GvHD. To validate the mini-endoscopically based grading system, histopathological studies were performed by using a previously reported microscopic grading system12. The data in Figure 4B confirm that the colon of mice severely affected by GvHD-related inflammation, as evidenced by high colonoscopic sum scores, display similarly strong histopathological signs of inflammation, given a histopathological sum score of ≥2 postmortem. In contrast, colon tissues of control mice display no (score 0) or, at most, mild (score 1) histopathological signs of inflammation, in line with the virtual absence of mini-endoscopically detectable signs of colitis. Furthermore, as shown in Figure 4C, D, correlation studies between mini-endoscopically and histopathologically assessed colitis activity and systemic GvHD scores were performed. Importantly, these studies demonstrated that mini-endoscopically determined sum scores of ≤3 reliably predict the absence of mid-to-higher grade (i.e., ≥2) intestinal GvHD-associated colonic inflammation scores obtained from histopathological grading. Finally, the severity of endoscopically assessed intestinal GvHD shows a correlation with the systemic GvHD activity.
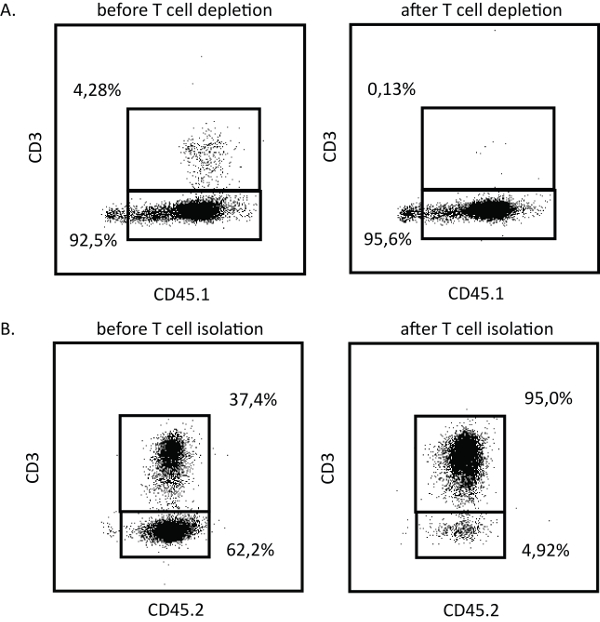
Figure 1: Flow cytometric quality assessment of magnetically purified T-cell-depleted bone marrow cells and allogeneic splenic CD3+ T cells. (A) Depletion of CD90.2+ bone marrow cells achieved by magnetic separation, using a commercially available purification kit. The purity of T-cell-depleted bone marrow cells was determined by flow cytometry, by staining cells prior to and after T cell depletion with anti-CD45.1 and anti-CD3. Results from one representative experiment are shown. (B) Splenic T cells were magnetically purified, employing a commercially available purification kit. The purity was determined by flow cytometry, comparing the frequencies of CD45.2 and CD3 costaining of samples derived from before and after T cell isolation. Results from one representative experiment are shown. Please click here to view a larger version of this figure.
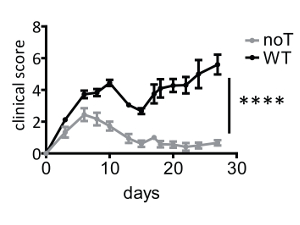
Figure 2: Clinical course of GvHD, employing an MHC class I fully mismatched model. To induce acute GvHD, BALB/c mice were whole-body irradiated on day 0. The mice received T-cell-depleted bone marrow cells 24 h later (d1). On day 2, the mice were injected with allogeneic splenic CD3+ T cells (wild-type [WT]; n = 9). As a control, some mice received T-cell-depleted bone marrow alone (noT; n = 9). The mice were specifically assessed three times a week for the presence and severity of clinical symptoms of GvHD. The displayed data represent mean values ± SEM of the clinical scores obtained from individual mice of the indicated treatment group from two representative experiments. The data were analyzed by two-way ANOVA, followed by Bonferroni's multiple comparisons posttest. ****p < 0.0001 was considered significant. Please click here to view a larger version of this figure.
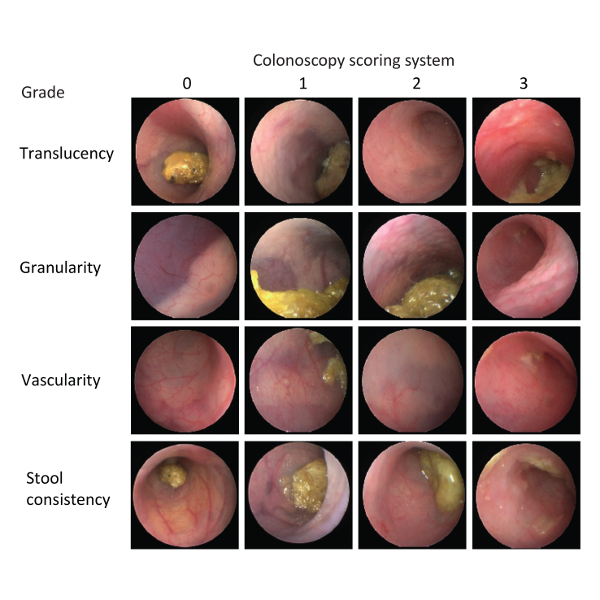
Figure 3: Representative images illustrating grading examples underlying the scoring matrix of the intestinal GvHD-related colon alterations assessed by a mini-endoscopic evaluation of the colons of live, allo-HCT-treated mice. To complement and illustrate the detailed description of the used scoring grading and system in Table 1, representative mini-endoscopic images of the evaluated severity levels (grading) for all parameters individually in the colon of anesthetized, live mice undergoing allo-HCT between days 26 and 30 before as described in Figure 1 are displayed here. Please click here to view a larger version of this figure.
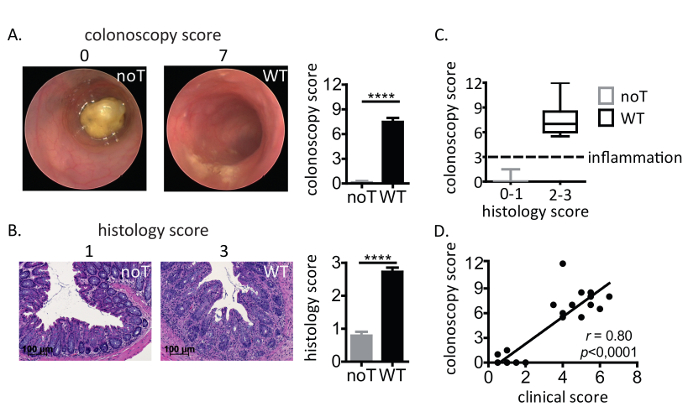
Figure 4: Mini-endoscopic scoring and grading of intestinal GvHD-related inflammation of the colon, reliably predicting the presence of higher-grade colitis assessed by histopathological scoring. (A) Between days 26 and 29 after the induction of GvHD as described in Figure 1, the manifestation of intestinal GvHD was evaluated by mini-endoscopy in live, anesthetized mice. Colonic alterations were scored and graded according to the scoring and grading system depicted in Table 1 and Figure 2. Representative endoscopic images of control (no T cell; noT) and wild-type (WT), T-cell-receiving mice and the mini-endoscopically assessed score (top) are shown. (B) The mice were sacrificed 12 h after the mini-endoscopic evaluation, and the distal part of the colon was processed and histopathologically assessed. The inflammatory activity of hematoxylin- and eosin-stained cross sections of the distal colon was graded. Representative hematoxylin- and eosin-stained cross sections of the distal colon of no T-cell- and WT T-cell-receiving allo-HCT-treated mice and the corresponding histology scores are shown. The data in panels A and B were analyzed by Student's t-test and are shown as mean ± SEM. ****p < 0.0001 was considered significant. WT: n = 15; noT: n = 15. The data represent pooled data from four individual experiments. (C) Interdependence of colonoscopy scoring and histological scoring. The data are shown as box plots. Each blot displays the median (black line within each box), the range of the data (min to max), and quartiles (areas of each box). WT: n = 15; noT: n = 15. The data represent pooled data from four individual experiments. (D) Correlation between colonoscopy scoring and clinical scoring. Both control and wild-type T-cell-receiving mice are included in the correlation analysis. The solid line represents the linear regression line. Spearman correlation coefficient (r-value) and p-value are shown. WT: n = 12; noT: n = 13. The data represent pooled data from three individual experiments. Please click here to view a larger version of this figure.
| Score | 0 | 1 | 2 | 3 |
| Translucency of the colonic wall | Extra-intestinal, inner organs (e.g. spleen) thoroughly visible | Discrete reduction of the visibility of extra-intestinal organs due to mild opacity of the colonic wall | Moderate reduction of the visibility of extra-intestinal organs due to significant opacity of the colonic wall | Lack of the visibility of extra-intestinal organs, i.e. non-transparent colonic wall |
| Granularity | Smooth, unaffected mucosal surface appearance; colonic crypt pattern visible | Discrete roughening and cobblestone appearance of the mucosal surface | Moderate roughening and cobblestone appearance of the mucosal surface | Severe roughening and cobblestone appearance of the mucosal surface; cushion-like appearance of the mucosa |
| Vascularity | Unaltered vascular pattern displaying the communicating network of large and small vessels | Discrete alterations of the vascular pattern; vessel pattern seems to fray | Some vessels are invisible; discontinuous vessel network | Contact induced bleeding; dot-like pattern of the vessels |
| Stool consistency | Normal; stool is hard; fine threads of mucus between feces and colonic wall can be observed |
Stool is still shaped but may contain ragged edges; deformable with the tip of the endoscope | Stool is soft and unshaped stool is visibly more shining (higher water content) |
Stool is loose, liquid; watery diarrhea. Stool may be randomly spread over the mucosal surface of the colon |
Table 1: Mini-endoscopic scoring and grading matrix of intestinal GvHD-related lesions in the colon of live allo-HCT-treated mice. Alterations of the endoluminal and transmural colon morphology in allo-HCT pretreated mice were assessed by a colonoscopy of the rectum and the distal colon of anesthetized, live mice, using a murine mini-endoscopy system. Colonic lesions were classified with the help of the endoscopic scoring system (modified murine endoscopic index of colitis severity [MEICS]) that is deduced from the original MEICS scoring system reported by Becker et al.9 and adapted to the context of allo-HCT. The distal colon is visually assessed for the presence and magnitude of the following four parameters: 1. the transmittance of endoscopic light (translucency) through the colonic bowel wall as thickening of the wall; 2. the mucosal surface displaying a cobblestone appearance (granularity) of the endoluminal-oriented mucosal surface; 3. an altered vascularization pattern (vascularity); 4. endoscopically assessed stool appearance in situ (stool consistency). Each parameter is scored from 0 (no signs) to 3 (most severe phenotype), adding up to a maximum sum score of 12 per mouse.
