Using the above-described image acquisition protocol, the first step is to visualize the left atrial appendage (LAA) using 2D acquisition (Figure 1). The probe is in the upper (or mid) transoesophageal position at 20-45°. The image shows the LAA. The left lateral ridge and the left upper PV is displayed at 60-80° (Figure 2), and then the 3D dataset is acquired and confirmed by cropping the dataset in order to visualize the LAA and the left lateral ridge with the left upper PV ostium (Figure 3). If the dataset does not encompass the whole structure of the LAA and the left lateral ridge, the image acquisition is repeated while changing the probe angulation, flexion or changing the patient position.
The next step is to visualize the left PVs. The probe angulation is changed to at around 120° to centralize the image to the LAA, and then the probe is turned slightly counterclockwise while moving the probe head to anteflexion. When the left PV ostium is visible (Figure 4), color Doppler is used to confirm that both the upper and lower PV is visible (Figure 5). Then the 3D dataset is acquired and confirmed by cropping the image to left upper and lower PV ostia with the intervenous ridge (Figure 6). If the dataset does not encompass the whole structure of the left PV ostium, image acquisition should be repeated while changing the probe angulation, flexion or changing the patient position.
The next step is the visualization of the right PVs. The probe angulation is changed to approximately 45° to centralize the image to the LAA, and then the probe is turned slightly clockwise while moving the probe head to anteflexion. When the right PV ostium is visible (Figure 7), color Doppler-coded imaging is used to confirm that both the upper and lower PV is clearly visible (Figure 8). Then the 3D dataset is acquired and confirmed by cropping the image to the right upper and lower PV ostia with the intervenous ridge (Figure 9 and Figure 10). If the dataset does not encompass the whole structure of the right PVs ostia, image acquisition should be repeated while changing the probe angulation, flexion or changing the patient position.
The next step is to prepare the 3D dataset offline and perform the measurements. The selected 3D dataset is opened in a dedicated platform-specific or a vendor-independent software for multiplanar reconstruction of the 3D images. First, one should select a frame timed to the T wave, and then two perpendicular planes are positioned to the PV ostia. The 3rd plane represents the en face view of the ostium (Figure 11), which is suitable to measure dimensions (distances, area). If the two perpendicular planes are fitted to the ridge, the widths of the ridges can be measured.
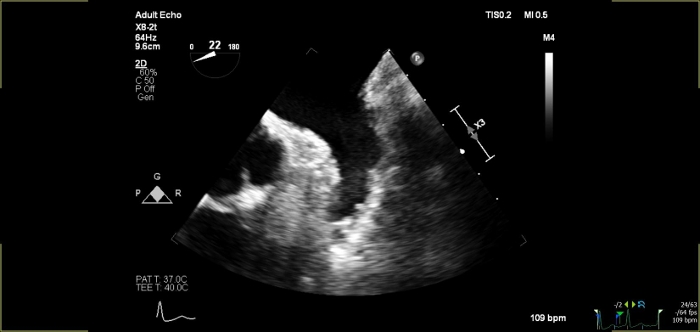
Figure 1: 2D view of the left atrial appendage at 22°.
Left atrial appendage Please click here to view a larger version of this figure.
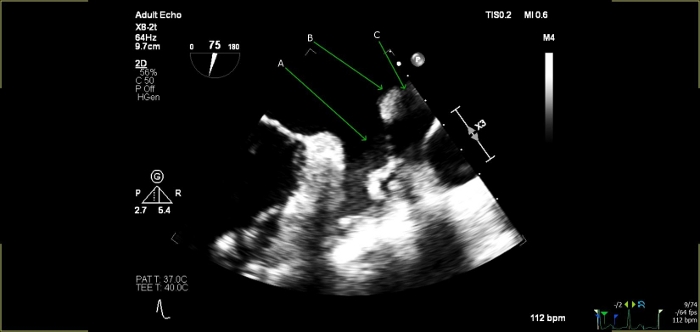
Figure 2: 2D view of the left atrial appendage at 75°.
(A) Left atrial appendage; (B) Left lateral ridge; (C) Left upper pulmonary vein Please click here to view a larger version of this figure.
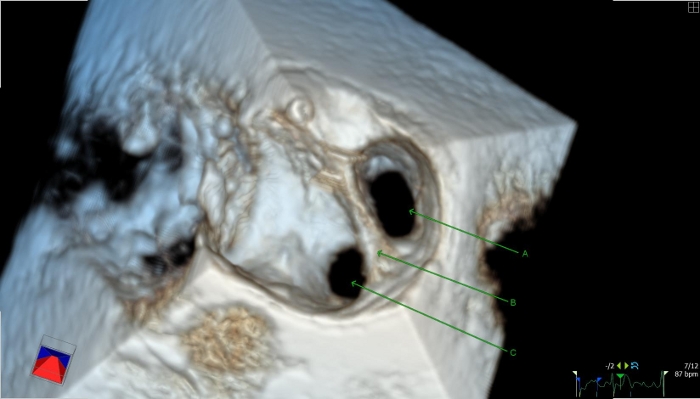
Figure 3: 3D reconstruction of the left lateral ridge and the left upper pulmonary vein.
(A) Ostium of the left upper pulmonary vein; (B) Left lateral ridge; (C) Left atrial appendage Please click here to view a larger version of this figure.
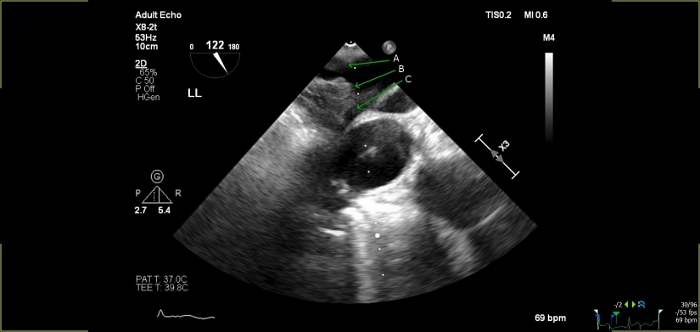
Figure 4: 2D view of the left pulmonary veins at 122°.
(A) Left lower pulmonary vein; (B) Intervenous ridge; (C) Left upper pulmonary vein Please click here to view a larger version of this figure.
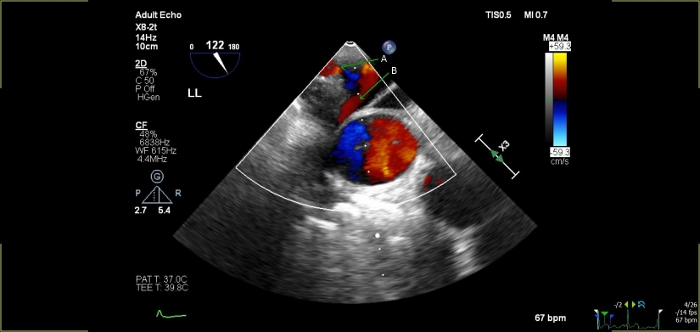
Figure 5: 2D color-coded image of the left pulmonary veins at 122° to confirm pulmonary venous flow.
(A) Left lower pulmonary vein; (B) Left upper pulmonary vein Please click here to view a larger version of this figure.
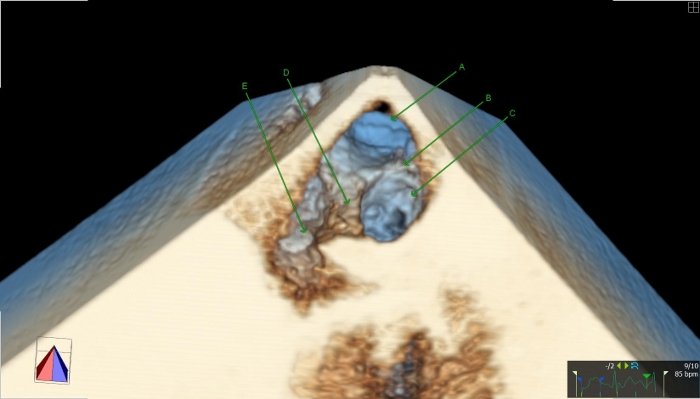
Figure 6: 3D reconstruction of the left pulmonary veins.
(A) Ostium of the left lower pulmonary vein; (B) Intervenous ridge; (C) Left upper pulmonary vein; (D) Left lateral ridge; (E) Left atrial appendage Please click here to view a larger version of this figure.
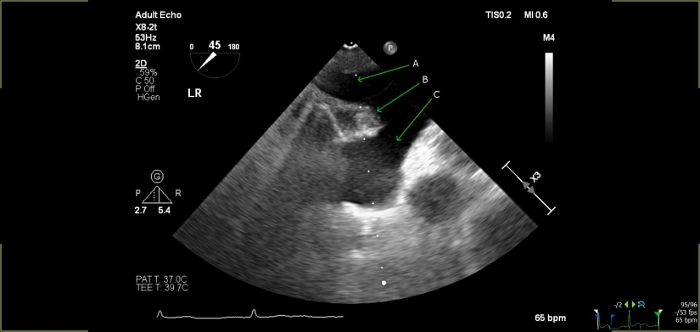
Figure 7: 2D view of the right pulmonary veins at 45°.
(A) Right lower pulmonary vein; (B) Intervenous ridge; (C) Right upper pulmonary vein Please click here to view a larger version of this figure.
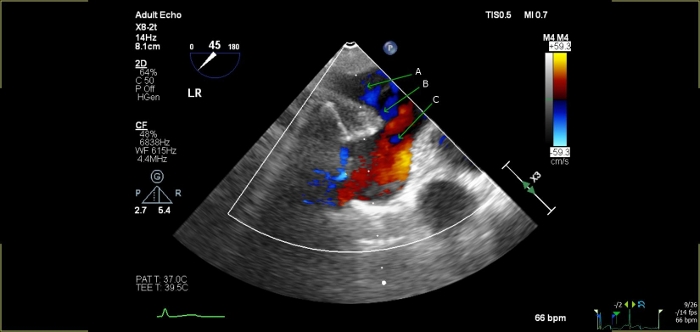
Figure 8: 2D with color-coded image of the right pulmonary veins at 45° to confirm pulmonary venous flow.
(A) Right lower pulmonary vein; (B) Intervenous ridge; (C) Right upper pulmonary vein Please click here to view a larger version of this figure.
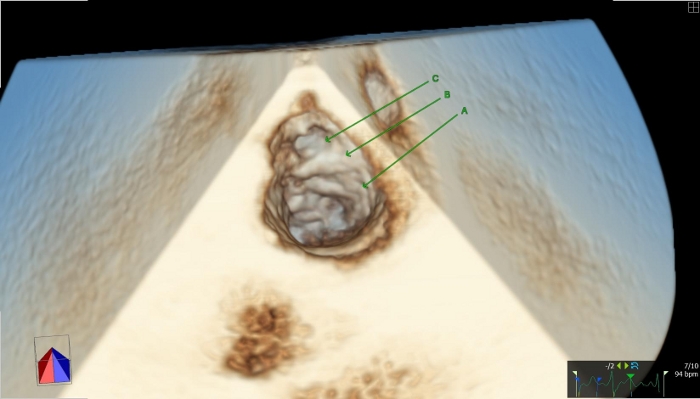
Figure 9: 3D reconstruction of the right pulmonary veins focusing on the right upper vein.
(A) Right upper pulmonary vein; (B) Intervenous ridge; (C) Right intermediate pulmonary vein (example for a supernumerous drainage pattern on the right side) Please click here to view a larger version of this figure.
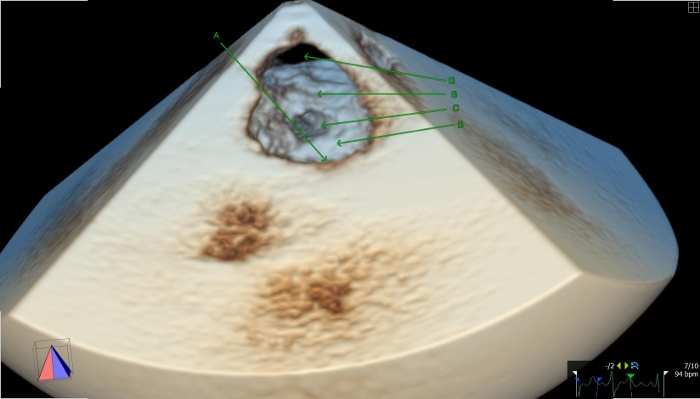
Figure 10: 3D reconstruction image of right pulmonary veins tilting the focus toward the right lower PV.
(A) Right upper pulmonary vein; (B) Intervenous ridge; (C) Right intermediate pulmonary vein (example for supernumerous drainage pattern in the right side); (D) Right lower pulmonary vein Please click here to view a larger version of this figure.
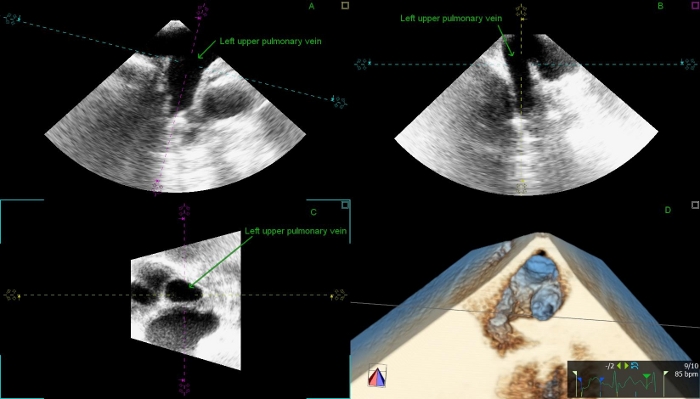
Figure 11: Multiplanar reconstructed 3D images of the left upper pulmonary venous ostium.
(A,B) Two perpendicular planes show the left upper PV longitudinally. The dotted lines represent the cutting planes. The blue one was fitted to the PV’s ostium. (C) Short axis view shows the en face view of the left upper pulmonary vein; (D) 3D dataset with a cutting plane. Please click here to view a larger version of this figure.
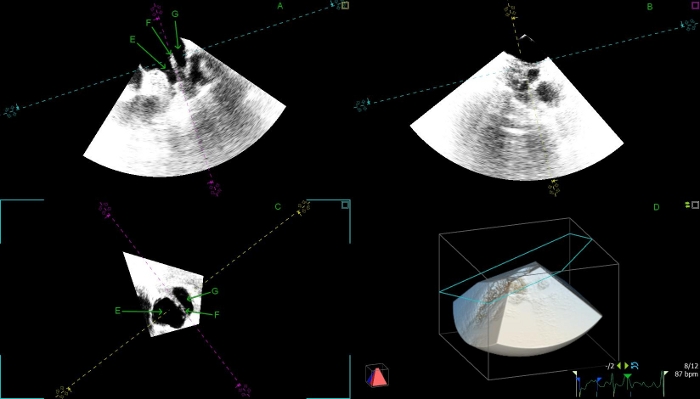
Figure 12: Multiplanar reconstructed 3D images of the left lateral ridge and left upper pulmonary vein.
(A) Left atrial appendage (longitudinal view – panel A; cross-sectional view – panel C); (B) Left lateral ridge (longitudinal view – panel A; cross-sectional view – panel C); (A) Left upper pulmonary vein (longitudinal view – panel A; cross-sectional view – Panel C) Please click here to view a larger version of this figure.
