The Institutional Review Board at The College of St. Scholastica has approved the study under which this protocol was developed and tested.
1. Fabrication of the visual screen
- Cut the ¾ inch (1.9 cm) diameter PVC pipe into various lengths: two 30 inch (76.2 cm) pieces (screen base); two 8 inch (20.3 cm) pieces (screen base); one 44 inch (111.8 cm) piece (vertical screen support); and one 32 inch (81.3 cm) piece (screen fabric holder).
- Place an end cap on one end of each 30 inch (76.2 cm) piece, and a 90° PVC elbow on the other end. Insert 8 inch (20.3 cm) pieces into the remaining open ends of both elbows. Connect open ends of the two 8 inch (20.3 cm) pieces with the PVC tee to create a screen base.
- Insert the 44 inch (111.8 cm) PVC piece into the vertical portion of the PVC tee to create a vertical support for screen. Place the 45° PVC elbow on the open end of the 44 inch (111.8 cm) piece. Insert the 32 inch (81.3 cm) piece into the open end of the 45° PVC elbow to create a screen fabric holder. Place an end cap on the open end of the 32 inch (81.3 cm) piece.
- Place dishtowels on top of one another to ensure fabric opacity. Secure to the 32 inch (81.3 cm) piece with athletic tape. The fully assembled screen can be seen in Figure 1.
2. Preparation of the testing equipment
- Calibrate electrogoniometer and electromyography (EMG) sensors according to the manufacturers’ instructions.
- Turn on the continuous passive motion (CPM) machine and activate Extension/Flexion mode. Program the CPM machine to move through 90° to 130° of elbow extension at a speed of 0.23°/s.
3. Preparation of the participant for TDPM testing
- Seat the participant in a standard height chair (18 inch/45.7 cm), ensuring sitting with a straight back and feet flat on floor.
- Verbally prepare the participant for the EMG sensor and the electrogoniometer placement using a standardized script: “To begin, I am going to prepare your skin to attach sensors. They will help record movement and ensure your muscles are relaxed during the test. I’m going to mark landmarks on your arm and start attaching the sensors, so you can just relax in the position I place you in.”
- Attach the biceps brachii and the triceps brachii EMG sensors.
- Manually resist elbow flexion to locate the biceps brachii muscle belly and mark the central point of the muscle belly with a small dot of washable marker to denote the location for the EMG sensor placement. Prepare the skin by removing the dead skin cells followed by scrubbing with an alcohol swab, and then attach the EMG sensor.
- Manually resist elbow extension to locate the muscle belly of the lateral head of the triceps brachii and mark the central point in the bulk of the muscle belly with a small dot of washable marker to denote the location for the EMG sensor placement. Prepare the skin by removing dead skin cells followed by scrubbing with an alcohol swab, and then attach the EMG sensor.
- Test the EMG function by evoking an isometric biceps brachii contraction, followed by an isometric triceps brachii contraction, and observing for EMG activation.
- Attach the electrogoniometer to the participant.
- Determine the midpoint of the dorsal aspect of the wrist and mark with a washable marker.
- Palpate the most prominent aspect of the lateral epicondyle and mark with a washable marker.
- Palpate the greater tubercle of the humerus and mark with a washable marker. Verify the greater tubercle location by passively moving the testing arm through internal and external rotation of the humerus as needed.
- Attach one end of the string to the lateral epicondyle mark using paper tape. Pull the string taut, connecting it with the dorsal wrist midpoint mark.
- Trace a line along the proximal forearm in line with the string using a washable marker.
- Move the free end of the string to the greater tubercle mark and pull the string taut.
- Trace a line along the distal humerus in line with the string using a washable marker, and then remove the string.
- Place the distal paddle of the electrogoniometer along the path of the traced line, 1.5 inches (3.8 cm) distally from the lateral epicondyle mark.
- Place the proximal paddle of electrogoniometer along the path of the traced line, 1.5 inches (3.8 cm) proximally from the lateral epicondyle mark. Secure the remaining components of the electrogoniometer to the skin using paper tape.
- Position the participant’s upper extremity comfortably in the CPM machine.
- Adjust the height and orientation of the CPM machine to achieve a position of 90° sagittal plane shoulder flexion, 90° elbow flexion, and a neutral forearm. Align the participant’s lateral epicondyle with the rotational axis of the CPM machine.
- Adjust the CPM machine hand support to fit comfortably with the palm of the participant’s hand and secure the forearm via a wrist strap. Figure 1 shows the final participant setup for TDPM testing.
4. Administration of the TDPM test
- Inform the participant of the testing procedure with the following standardized verbal information: “During this test, the machine is going to move very slowly to either straighten or bend your elbow. We will say “begin” at the start of each trial, there will be eight trials. When I say begin, the machine may or may not move your arm. Please press the button as soon as you feel your arm move, but only when you feel movement. If you don’t feel movement, we will stop the trial after a period of time; try to pay attention until we stop the trial. This is the button you’ll be using. Please press the button right now to test it.”
- Hand the participant the electrogoniometer event marking trigger switch and test the switch.
- Inform the participant of additional aspects of the procedure: “In between each trial, whether your arm moved or not, we will take your arm out of the machine and straighten it, and then place it back in the machine. Please remain relaxed. Do you have any questions about the test? We will be using this curtain to block your vision during this test and place this hearing protection over your ears to minimize any sounds you might hear during the testing.”
- Occlude visual input by blocking the view of the arm being tested and the CPM machine using a visual screen. Drape screen material at the participant’s shoulder to avoid sensory input during arm movement. Diminish auditory input by placing noise-cancelling headphones on the participant (see Figure 1).
- Loudly state “begin,” and wait the corresponding amount of time per trial before initiating movement of the CPM machine to decrease participant guessing when movement will begin19. Standardized delay times are shown in Table 1.
| Trial Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Delay (s) | 1 | Catch | 3 | 1 | 2 | Catch | 3 | 1 |
Table 1: Standardized time delays and catch trial locations. Varied trial start time delays are included to prevent participant attempts to guess when movement will begin. Catch trials are included to test whether or not participant is actually detecting movement19,31.
- Observe for activation of biceps brachii and triceps brachii muscles by monitoring EMG sensor feedback readings to ensure that the participant does not attempt to use active movement to assist in movement detection.
- If muscle activation is noted, stop the trial and use the following standardized script: “Your muscles are activating. Please try to keep your arm relaxed during the test.” This trial should be noted for exclusion from data analysis, with the researcher proceeding with resetting the participant and CPM to start the next trial (protocol step 4.7).
- Between each trial, remove the participant’s testing arm from the CPM machine and return the CPM machine to a 90° start position. Passively move the participant’s elbow through full extension and then back to 90° flexion to standardize the muscle spindle movement history27,28. Place the arm back in the CPM machine for the next trial.
- Complete eight trials, including two “catch” trials where the participant’s arm is not moved19. Terminate each trial (catch and non-catch) when the participant depresses the trigger switch, or after 15 seconds if the trigger switch is not depressed.
- If during a catch trial a participant verbally reports they cannot feel movement, or depresses the trigger switch, use the following standardized response: “Your arm did not actually move during that trial. I know it’s hard to feel, the machine moves very slowly; try to concentrate and push the button as soon as you feel your arm move or that your arm position has changed.”
5. Calculation of participant’s TDPM score
- Using the electrogoniometer tracing, identify the electrogoniometer angle measurement for the point at which the CPM machine movement started, and for the point at which the participant depressed the trigger switch indicating movement was felt. See Figure 2 for a representative example.
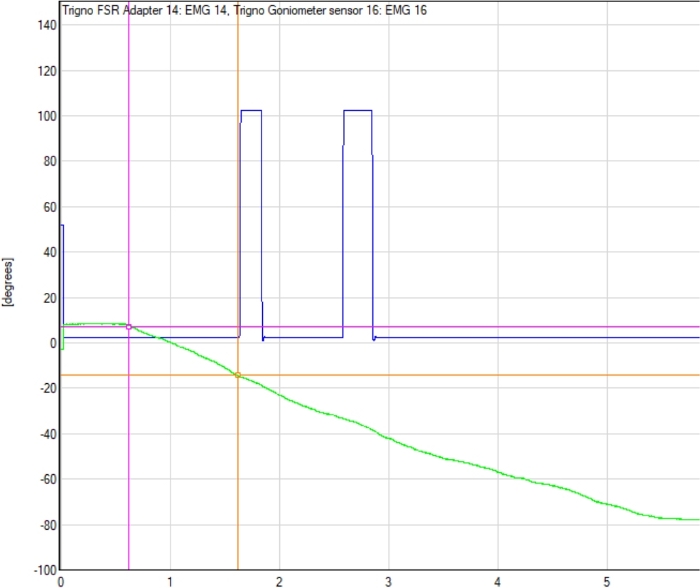
Figure 2: Example electrogoniometer tracing with detection point. The electrogoniometer line tracing (green line), start point of the continuous passive motion (CPM) machine movement, and the point at which participant indicated movement was detected (first blue peak) are shown. The difference between electrogoniometer readings at the start of the trial (pink circle) and at detection point (orange circle) determines the TDPM value for that trial. Please click here to view a larger version of this figure.
- Subtract the starting angle from the final angle, thus identifying the number of degrees the CPM moved; this is the participant’s elbow TDPM value for that trial.
- To determine participant’s overall TDPM score, remove the smallest and largest TDPM values from the six non-catch trials, and then average the remaining four trial scores29.
Participants:
Using the protocol presented here, elbow TDPM was measured in an academic research laboratory for two different groups of individuals: 20 healthy adults, and eight adults with chronic stroke. Participants for both groups were recruited from the community using fliers, emails, and word-of-mouth. The healthy adults (14 females, six males; mean age (SD) = 28 (7.9) years; 19 right- and one left-handed) were tested to generate representative results for an unimpaired population. Inclusion criteria were: age of 18 to 85 years; ability to follow two-step directions as determined by screening at initial meeting. Exclusion criteria were: history of disease or conditions affecting neuromuscular function of the upper limbs based upon self-report; reported allergy to metal or latex. Handedness was assessed using the Edinburgh Handedness Inventory30. Half of the healthy adult participants had TDPM of their right elbow tested, and half had their left elbow tested (block randomization). To determine the test-retest reliability of this protocol, healthy adult participant elbow TDPM was measured twice, one week apart. The tBKT was completed on Day 1 following TDPM testing. No adverse events occurred for any participant in the healthy participants group.
The elbow of the ipsilesional (i.e., less affected) upper limb of the individuals with chronic stroke (five males, three females; mean age (SD) = 69 (11.3) years; five right hemisphere stroke, three left hemisphere stroke) was tested to represent the protocol’s capability for detecting and quantitatively discriminating TDPM in individuals with suspected mild proprioceptive impairment. Inclusion criteria for this group were the same as for the healthy adult group, with the addition of: history of stroke occurring more than six months prior that impacted upper extremity function. Exclusion criteria were: any history of ipsilesional upper extremity pain or musculoskeletal injury; reported allergy to metal or latex. Participants with chronic stroke completed one elbow TDPM testing session. The tBKT was completed following elbow TDPM testing. One participant with stroke reported mild irritation from the EMG sensor adhesive; no other adverse events occurred.
Results:
No statistical difference was found between right and left elbow TDPM scores for healthy adults (p = 0.86, two-tailed); the data was combined for subsequent analyses. The average elbow TDPM for healthy adult participants (n = 20) was 1.19 (±1.02) degrees. The Spearman correlation and intraclass correlation coefficient (ICC) were calculated to evaluate test-retest reliability of the TDPM; a positive and statistically significant relationship was found (rs = 0.72, p < 0.001), (ICC 2,4 = 0.84), suggesting moderate to good reliability of the measure among healthy adult participants24 (Figure 3).
The average ipsilesional elbow TDPM for participants with chronic stroke (n = 8) was 8.24 (±4.53) degrees (Table 2). Participants with chronic stroke were more variable than healthy adult participants (Figure 4A). Using a two-tailed t-test, the TDPM of the healthy adult and chronic stroke groups were found to be statistically different, with the adults with chronic stroke requiring a greater elbow extension excursion prior to movement being detected (t = 4.4, p = 0.003, two-tailed) (Table 2). Spearman correlation between elbow TDPM and error in targeted reaching as measured by the tBKT showed a moderate relationship between these two measures (rs = 0.63, p < 0.001) (Figure 5). Participant tBKT scores are shown in Figure 4B.

Figure 1: Participant setup for elbow threshold to detection of passive movement (TDPM) testing. The continuous passive motion (CPM) machine extended the participant’s elbow at a constant speed of 0.23°/s. Note the visual screen placed to occlude vision of the testing arm. Not visible are hearing occlusion headphones, and a trigger switch for participant indication of movement detection. Please click here to view a larger version of this figure.
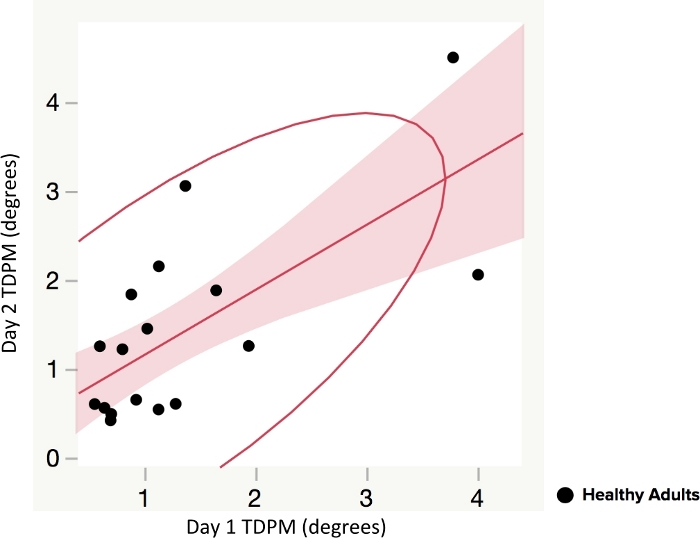
Figure 3: Test-retest reliability of elbow threshold to detection of passive movement (TDPM) method in healthy adults. Spearman correlation and intraclass correlation coefficient (ICC) of Day 1 and Day 2 (tested one week apart) were used to compare TDPM scores. Figures show line of fit with 95% confidence interval (shaded area) and a density ellipse. A positive and statistically significant relationship was found (rs = 0.72, p < 0.001). Please click here to view a larger version of this figure.
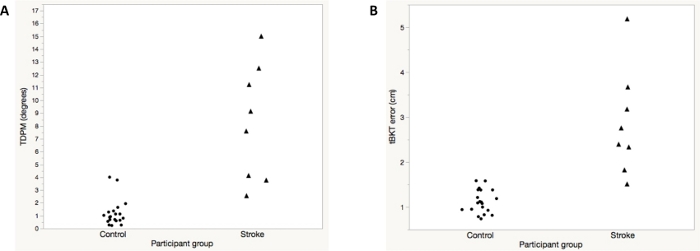
Figure 4: Representative results for elbow threshold to detection of passive movement (TDPM) (A) and the tablet version of Brief Kinesthesia Test (B) for healthy adult control subjects versus participants with chronic stroke. Note that one individual with chronic stroke was unable to detect movement on any trial; the maximum specified TDPM value of 15° was assigned. This same individual had the greatest amount of error during tBKT testing. Please click here to view a larger version of this figure.
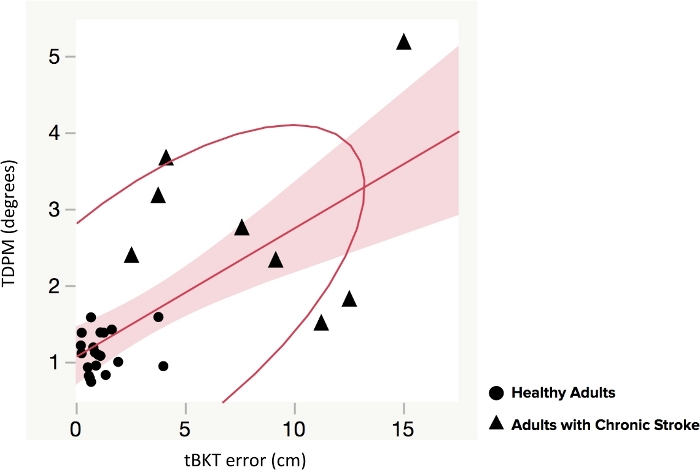
Figure 5: Elbow threshold to detection of passive movement (TDPM) scores compared to tablet version of the Brief Kinesthesia Test (tBKT) scores in healthy adults and adults with chronic stroke. Spearman correlation between elbow TDPM and error in targeted reaching as measured by the tablet version of the Brief Kinesthesia Test (tBKT) is shown. There was a moderate positive relationship (rs = 0.63, p < 0.001). Please click here to view a larger version of this figure.
| Age | Sex | Stroke Chronicity | Handedness | Fugl-Meyer | TDPM | tBKT Error | |
| Mean(SD) in years | Mean(SD) in months | Mean (SD) of shoulder-elbow subscore/36 | Mean (SD) in degrees | Mean (SD) in cm | |||
| Healthy adults (control) n = 20 | 28(7.9) | 14 F; 6 M | NA | 19 – R 1- L | NA | 1.19 (1.02) | 1.12 (0.26) |
| Adults with chronic stroke n = 8 | 69(11.3) | 3 F; 5 M | 33(19) | 7 – R 1- L | 23.9(8.5) 5 – R CVA 3 – L CVA | 8.24 (4.53) | 2.85 (1.16) |
| SD = Standard deviation; F = Female; M = Male; R = Right; L = Left; CVA = Cerebrovascular Accident; NA = Not applicable; cm = centimeter | t = 4.4, p = 0.003 (two-tailed) | t = 4.15, p = 0.004 | |||||
Table 2: Participant description, average elbow threshold to detection of passive movement (TDPM) scores (degrees), and average tablet version of the Brief Kinesthesia Test (tBKT) scores. A significant difference was found in average elbow TDPM between healthy controls and adults with chronic stroke, as well as in the average tBKT scores.
