All presented data, except FACS plots, were analyzed with a statistics software. The FACS plots were analyzed using flow cytometry software.
The analysis of whole blood cell count did not show any significant differences with respect to erythrocytes between all tested conditions (Figure 2). But, platelets and leukocytes were drastically reduced in the latex group, indicating a very poor biocompatibility of latex. This is further underlined by increased levels of free hemoglobin in the latex group, indicating the fact that except for the latex group, none of the other vascular devices or conditions led to extensive hemolysis (Figure 2). Further, the coated PVC tubes, polyPVC and hepPVC, as well as the tested stent did not lead to thrombosis by means of platelet and leukocyte loss, while latex exhibited the highest platelet and leukocyte loss, followed by uncoated PVC tubes that showed a decreased trend.
While all the tested vascular devices led to increased activation of the coagulation system (FPA) and complement component (sC5b-9), the hepPVC loops exhibited a trend for decreased levels of FPA and sC5b-9 when compared specifically to polyPVC loops (Figure 3). Interestingly, uncoated PVC and Gap loops showed lower levels of FPA compared to polyPVC, though not reaching the level of statistical significance. Nevertheless, latex loops exhibited significantly increased levels of FPA when compared to baseline and static conditions.
In accordance with the whole blood cell counts, latex loops exhibited highest levels of TNF, IL-6 and PMN elastase (Figure 4), reaching the level of statistical significance when compared to rest of the groups in terms of TNF and IL-6 (Figure 4A,B), whereas to static and baseline conditions in terms of PMN elastase (Figure 4C). These results indicate the potent activation of leukocytes by latex. The baseline levels of activation markers were always comparable to static conditions, indicating a proper heparinization of the blood.
Interestingly, it was shown that platelet and leukocyte counts for gap induced loops were only slightly reduced with moderate activation of the coagulatory system (FPA) and leukocytes (PMN elastase), though improper loop closure with resulting flow turbulences and blood contact to the uncoated, rough cutting surface led to macroscopically visible clots at the splice (Figure 1F). The clots and its distribution over the whole splice surface were evident with µCT and SEM images, while no clot was found when the loops were closed with the external closing device leaving no gap between the loop endings (Figure 5).
Flow cytometric analysis of host blood cells that were stained with platelet specific markers, CD41 and platelet activation marker CD62P, are shown in Figure 6A,B. Here, the latex tubes exhibited exceedingly high median fluorescence intensity (MFI) for CD62P on blood platelets, followed by stent, whereas heparin coated polyPVC tubes exhibited minimal activation of platelets depicting anti-thrombogenic property of polyPVC tubes. Furthermore, leukocytes were classified based on the CD45 and SSC (side scatter) based granularity into (i) granulocytes; (ii) monocytes and (iii) lymphocytes (Figure 7), and the expression of CD162+ integrin was detected on each subpopulation of leukocytes that are known to interact with the CD62P on platelets24. It was noticed that the integrin expressions were drastically reduced on granulocytes and lymphocytes in latex loops. This result was in line with lowered levels of total frequencies of leukocytes in the latex loops (Figure 2). In general, the integrin levels were higher among monocytes when compared to granulocytes and lymphocytes, indicating the likelihood for the monocyte interaction with activated platelets. In this regard, monocyte platelet aggregates were also evaluated by staining the blood cells with CD14 (as monocyte marker) and CD41 (as platelet marker) and ultimately to identify double positive cells i.e. CD14+CD41+MPA (Figure 8). Here, we noticed that the stent group exhibited the highest levels of CD41 expression on the MPA, followed by the latex group, indicating an increased tendency to form MPA, despite the reduced frequency of monocyte (<1 %) in the latex loops.
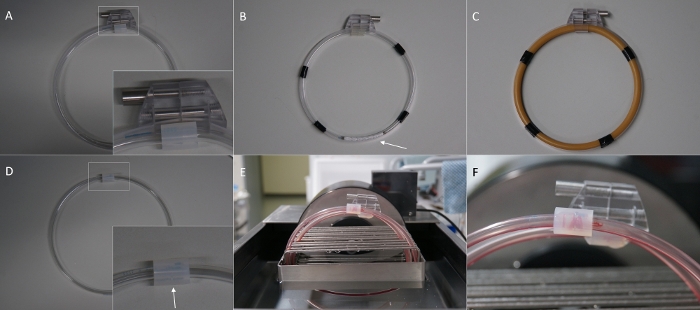
Figure 1: Overview of the in vitro hemodynamic loop model and its modifications. (A) Loop for the gap experiment with external loop closing system, leaving no gap at the splice. (B) Loop made of polyPVC coated PVC tube and stent inside (arrow). (C) Loop made of latex tube. (D) Loop for the gap experiment without the external loop closing system leaving a gap between the tube endings (arrow). (E) Loops placed in the loop cradle inside the water bath and filled with blood. (F) Thrombus resulting in a gap at the splice (arrow) after rotation. Please click here to view a larger version of this figure.

Figure 2: Results for blood cell count and plasma hemoglobin. (A) Erythrocytes count. (B) Platelets count. (F) Leukocytes count. (D) Free plasma hemoglobin. The results indicate the poor biocompatibility of latex, leading to excessive hemolysis. Data are presented as mean value; error bars indicate SEM. n=1. Please click here to view a larger version of this figure.
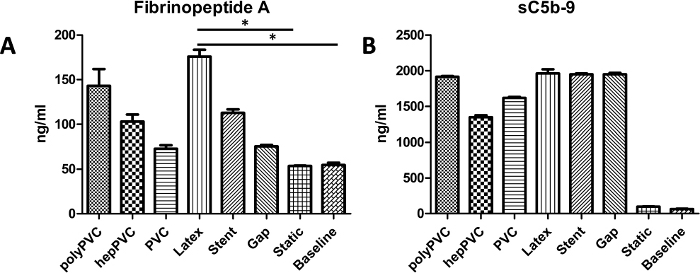
Figure 3: Results for activation of the coagulation and complement system. (A) Coagulation system activation, measured by levels of Fibrinopeptide A (FPA) (B) Complement system activation, measured by levels of sC5b-9. While latex tubes evoked significant elevated levels of the FPA, the complement activation was strong for all tested materials. Data are presented as mean value, error bars indicate SEM. *p<0.05, n=1. Please click here to view a larger version of this figure.
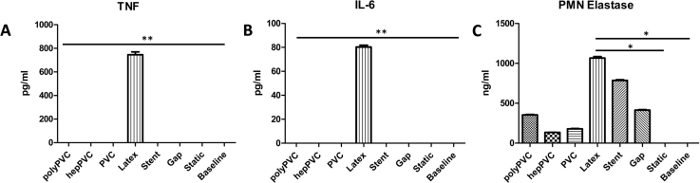
Figure 4: Leukocyte activation markers. (A) Tumor necrosis factor alpha (TNF). (B) Interleukin 6 (IL-6) (C) PMN Elastase. The results indicate increased activation of leukocytes due to elevated levels of the analyzed markers, followed by stent loops, that only led to increased levels for PMN Elastase but not TNF or IL-6. Data are presented as mean value, error bars indicate SEM. *p<0.5; **p<0.01, n=1. Please click here to view a larger version of this figure.
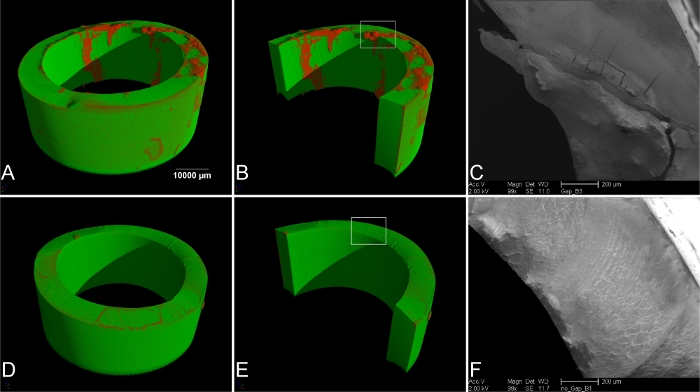
Figure 5: Imaging of the splice of the loops. (A) µ-computer tomography (µCT) of loops with improper closing (gap). The red areas indicate thrombus material. (B) Rendering of the luminal side of the tube. The rectangular selection indicates the area for scanning electron microscopy (SEM) (C). (D) µCT of loops with external loop closing device and no gap at the splice, and (E) rendering and view of the luminal surface. No thrombus material was found. (F) SEM image of the rectangular selection in (E). No thrombus material was found on the cutting surface. Please click here to view a larger version of this figure.
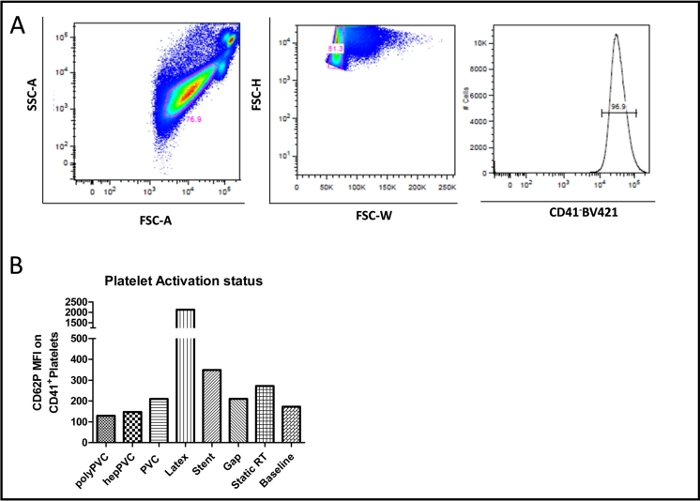
Figure 6: FACS plot for platelet activation (CD62P). (A) Representative FACS plot (basic condition) showing the blood CD41+ platelets. (B) Graph showing the platelet activation status reflected by the mean fluorescence intensity (MFI) of the different types of vascular devices in comparison to the static RT and baseline conditions. The data bars present data from single measurements. Please click here to view a larger version of this figure.
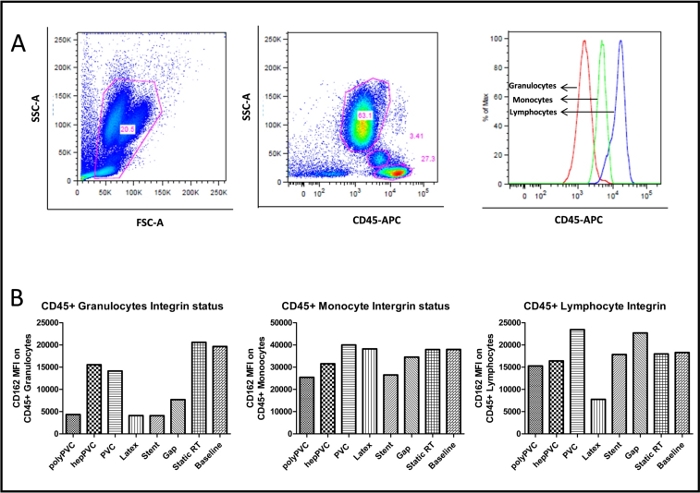
Figure 7: FACS plot for leukocyte integrin (CD162). (A) Representative FACS plot (basic condition) showing the blood CD45+ leukocytes and subgroups (B) Graph showing the leukocyte CD162+ integrin mean fluorescence intensity (MFI) of the different types of vascular devices in comparison to the static and baseline conditions. The data bars present data from single measurements. Please click here to view a larger version of this figure.
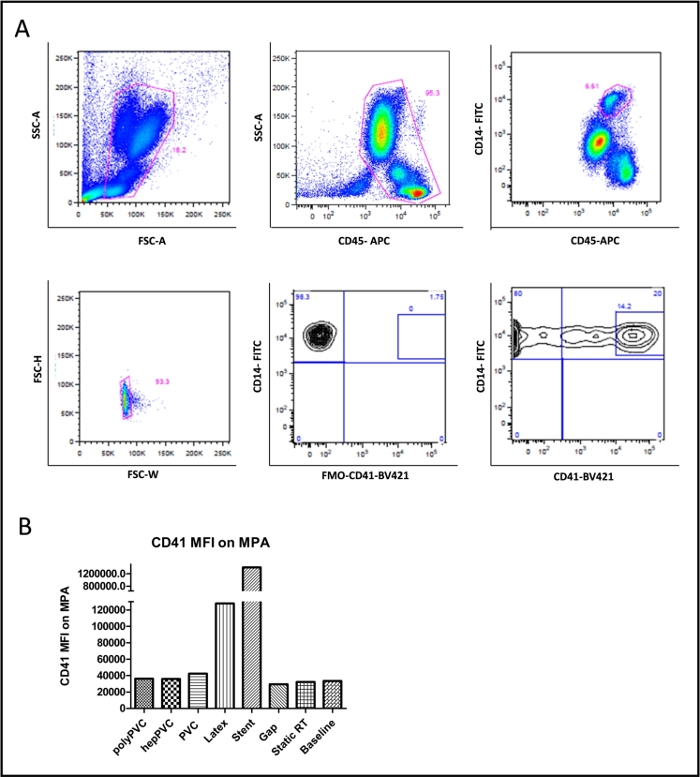
Figure 8: FACS plot for platelet monocyte aggregates (CD41/CD14). (A) Representative FACS plot (basic condition) showing the gating for blood monocytes (CD45+/CD14+), platelets (CD41+) and monocyte platelet aggregates (CD41+/CD14+) (B) Graph showing the CD41+ mean fluorescence intensity (MFI) on monocyte platelet aggregates for the various vascular devices compared to the static and baseline conditions. The data bars present data from single measurements. Please click here to view a larger version of this figure.