All human subject research was performed in accordance with the Institutional Review Board of the University of Nebraska-Lincoln, and informed consent was obtained from all subjects.
1. Locating the MCA signal by freehand TCD
NOTE: “Freehand” TCD refers to operation of TCD with a handheld transducer to find a CBFV signal before beginning an fTCD experiment.
- Setting TCD parameters
- Keep the power at a reasonably high value (e.g., 400 mW) during the initial search for the MCA. Once the MCA signal is located, reduce the power as much as possible while still maintaining a “good” signal (see step 2.2.7).
NOTE: Using a reasonably high power during the initial search does not violate the “As Low As Reasonably Achievable” (ALARA) principle of exposure to acoustic radiation because higher power will allow the MCA signal to be discovered more quickly10. - Set the sample volume to 8–12 mm during the initial search for the MCA signal. If the signal is difficult to find, increase the gate size to increase the intensity of the signal, but note that this may incorporate the signal from one or more nearby arteries into the signal from the MCA.
- Set the gain at a medium level, with the goal of “keeping background noise at a minimum, but present”10.
- Set the high-pass filter cutoff (normally termed “threshold”) to 50–150 Hz.
- If the subject is an adult, set the depth to 50 mm, which is the average mid-point depth of the M1 segment of the MCA10 (Figure 1).
NOTE: This setting will be discussed in more detail in subsequent steps. Depth settings for children are given in Table 1.
- Keep the power at a reasonably high value (e.g., 400 mW) during the initial search for the MCA. Once the MCA signal is located, reduce the power as much as possible while still maintaining a “good” signal (see step 2.2.7).
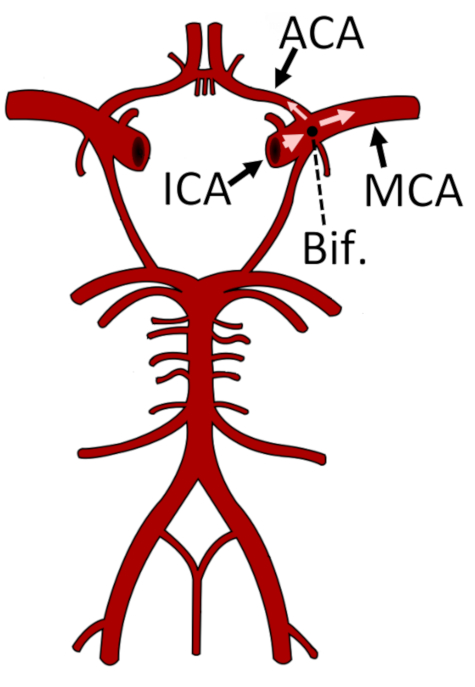
Figure 1: Representation of the circle of Willis and the major arteries of the cerebral circulatory system. The bifurcation of the ICA into the ACA and MCA is marked with a black circle. The M1 segment of the MCA is shown. This figure has been modified from24. Abbreviations: ACA = anterior cerebral artery; Bif. = bifurcation; ICA = internal carotid artery; MCA = middle cerebral artery. Please click here to view a larger version of this figure.
- Locating the temporal window
NOTE: The temporal window, also called the transtemporal acoustic window, is a part of the skull where the bone is thinnest11, thus allowing transmission of low-frequency ultrasound energy through the cranium (Figure 2).- For infants and small children, locate the temporal window just in front of the ear (the “intertragal space”) and above the rostral edge of the zygomatic arch, which can be easily felt under the skin.
- For teenagers and young adults, locate the temporal window via any of the subwindows.
NOTE: The posterior subwindow usually provides the best signal (Figure 2). - For adults aged 30 years or older, locate the temporal window just in front of the ear.
NOTE: The acoustic window decreases in size as people age due to increasing porosity of the bone of the cranium, causing some older people to have a very limited temporal window12. In such individuals, bilateral insonation of the MCA is sometimes impossible.
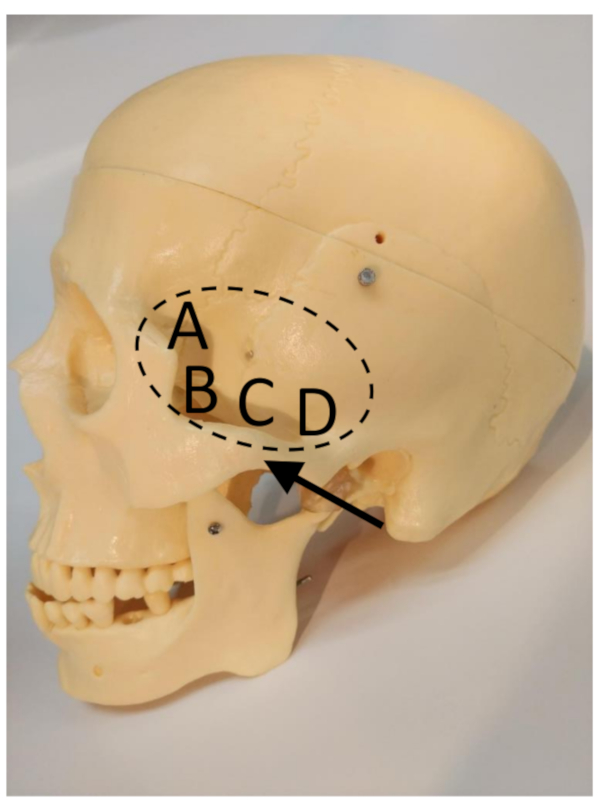
Figure 2: The transtemporal window (marked by the dashed ellipse), zygomatic arch (arrow), and subwindows11. (A) Frontal subwindow. (B) Anterior subwindow. (C) Middle subwindow. (D) Posterior subwindow. Please click here to view a larger version of this figure.
- Applying the transducer
- Apply enough ultrasound gel to cover the surface of the transducer.
NOTE: When placed on the head, the gel should cover sufficient space to maintain a seal between the scalp and the Doppler probe’s surface, thus preventing signal interruption from air coupling underneath the probe’s surface. - Alert the subject that the gel may feel cold (if at room temperature).
- Place the transducer on the temporal window, which was located in section 1.2.
- Apply enough ultrasound gel to cover the surface of the transducer.
- Searching for the MCA
- After placing the transducer on the scalp, search for the MCA signal, which will generally be located slightly anterior (forwards) and rostral (towards the head) from the location of the initial transducer scalp placement10.
- If the TCD spectral signal is not immediately obvious, adjust the angle of the transducer while keeping it in the same location relative to the scalp. Slowly angle the probe from rostral to caudal (towards feet) and posterior to anterior.
NOTE: Figure 3 shows two spectra taken from the same position, but at different angles. - If a signal is still absent after performing step 1.4.2, check the color M-mode display for flow in the MCA at different depths (indicated by red coloring). Increment or decrement the signal depth in 5 mm steps and search as described in step 1.4.2. If flow is visible in M-mode but not in the Doppler spectrum, increase or decrease the depth until the flow signal is visible in the Doppler spectrum.
- If a satisfactory signal is still not obtained, move the transducer to a nearby position on the scalp, which is slightly more anterior, and repeat steps 1.4.1–1.4.3.
- When an optimal MCA signal is obtained, note the depth and maximum velocity.
- Using a washable makeup pen, place a mark on the scalp (trace part of the transducer edge) where the optimal signal was found.
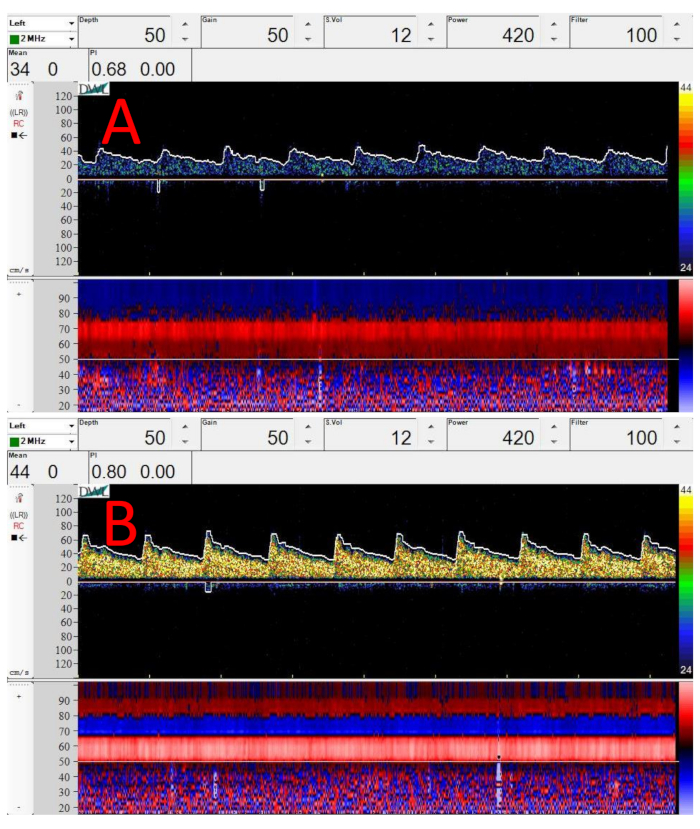
Figure 3: Sample Doppler spectra and M-mode images from midpoint of M1 segment of the MCA. (A) Spectrum taken right after applying transducer to the temporal window, just in front of the ear. (B) Sample Doppler spectrum at same location and depth as (A). The only change is that the transducer has been angled upwards (superiorly) slightly. In both (A) and (B), depth = 50 mm, gain = 50, sample volume = 12 mm, power = 420 mW/cm2, and filter = 100 Hz. Please click here to view a larger version of this figure.
- Searching for the bifurcation
NOTE: Finding the bifurcation of the internal carotid artery (ICA) is important to help confirm that the MCA is the artery being monitored. This step should be performed on both sides if bilateral monitoring will be performed, as the bifurcation may not be at the same depth on both sides.- Increase the depth until the signal from the bifurcation of the ICA into the MCA and ACA is noted (Figure 4), typically at a depth of 51–65 mm10.
- Search for the optimum bifurcation spectral signal using the procedure described in step 1.4.2. Always strive for the highest-velocity spectral signal possible10.
- When an optimal bifurcation signal is obtained, note the depth of the bifurcation.
- For bilateral monitoring, repeat sections 1.1–1.4 and steps 1.5.1–1.5.3 on the other side of the head.
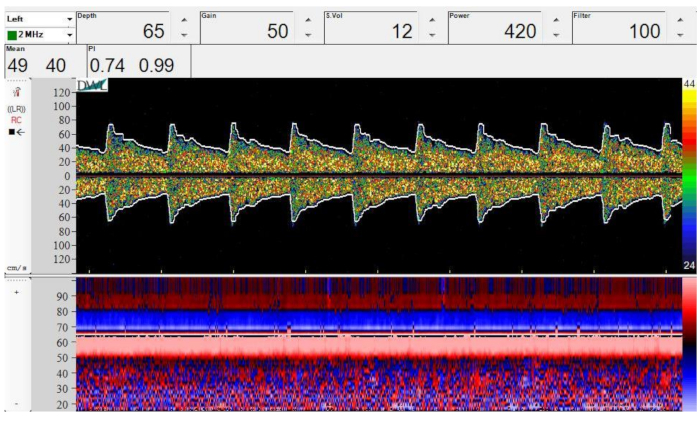
Figure 4: Spectral Doppler (top) and M-mode (bottom) image of bifurcation of the ICA into the MCA and ACA. Depth = 65 mm, gain = 50, sample volume = 12 mm, power = 420 mW/cm2, and filter = 100 Hz. Please click here to view a larger version of this figure.
2. Relocating the MCA after placing a fixation device
NOTE: For fTCD experiments, it is necessary to monitor CBFV for 10–90 min or longer. Therefore, a fixation device (Figure 5) is crucial to provide stability.
- Placing the fixation device
- By visual inspection, adjust the fixation device (Figure 5) to the subject’s approximate head size.
- Alert the subject before placing the headset on his or her head. Place the headset on the subject’s head.
NOTE: If the subject has long or thick hair, it may be necessary to tie the subject’s hair back, depending on the fixation device being used. - Adjust the fixation device’s fit, and ask the subject if the device is too tight.
NOTE: The device should be tight enough that it does not move when bumped slightly, but loose enough that the subject is not uncomfortable.

Figure 5: Subject wearing custom fixation device. Please click here to view a larger version of this figure.
- Locating the MCA signal
- Loosen the mechanism of the fixation device holding the transducer in place (e.g., loosen the mechanism, shown in in Figure 5, by turning a knob counterclockwise) so that the transducer can move freely.
- Alert the subject before applying gel to the transducers (which should already be in place from section 2.1), and that the gel may be cold (if it has been stored at room temperature).
- Apply enough ultrasound gel to the transducer to cover the face of the transducer.
- Adjust the fixation device so that the transducer is located over the top of the mark made in step 1.4.6.
- Search for the optimal MCA spectral signal using the procedure described in steps 1.4.1–1.4.3. Always strive for the highest-velocity spectral signal possible10.
NOTE: When compared to freehand TCD, the optimal depth at which the MCA is located using the fixation device may differ slightly (at most 1–2 mm) from the depth for the freehand device. This is because the fixation device may hold the transducer slightly further away from the scalp while still maintaining a coupling gel seal. - When the optimal MCA spectral signal is found, tighten the mechanism of the fixation device to lock the transducer in place. Note the depth and all other settings.
- Decrease the power (see step 1.1.1) as much as possible while still maintaining a spectral envelope that traces the maximal velocity accurately.
- For bilateral monitoring, repeat steps 2.2.1–2.2.7 on the other side.
3. Performing a breath-hold maneuver
NOTE: This section is given as an example of a functional experiment that may be performed using the experimental setup described in section 1 and section 2.
- Perform all steps described in section 1 and section 2.
- Begin recording on the TCD software.
- Breathe normally for 3 min to achieve a good baseline recording, and allow CBFV to stabilize from any previous experiments or stimuli.
- Count down slowly from three. On the count of one, ask the subject to begin breath-holding following a normal inspiration13.
NOTE: The subject should not inhale deeply, as this would decrease carbon dioxide in the lungs and decrease the likelihood of observing the increase in CBFV due to cerebrovascular reactivity. The subject should also avoid performing a Valsalva maneuver, in which intrathoracic pressure is substantially increased against a held inspiration14. - Place a marker in the TCD recording to signify the start of breath-holding.
- Have the subject hold their breath for 30 s, or until they are no longer comfortable holding their breath.
- When the subject inhales, place a marker in the TCD recording to signify the end of breath-holding.
- Continue monitoring CBFV using TCD and recording for at least 30 s following the end of breath-holding to ensure that CBFV returns to baseline values.
Figure 3 shows sample Doppler spectra and color M-modes from the midpoint of the M1 segment of the MCA. Figure 3A,B were taken at the same position on the scalp, but at different angles. Note how a very small change in angle, without changing the contact position on the scalp, can greatly improve Doppler signal strength, as shown by the higher-intensity yellow coloring of the spectrogram in Figure 3B. Note also that the M-mode in Figure 3B shows two arteries (blue and red, corresponding to the ACA and MCA, respectively).
Figure 4 shows a sample Doppler spectrum and M-mode from the bifurcation of the ICA into the ACA and MCA. Note the overlapping red- and blue-shaded regions in the M-mode image denoting the MCA and ACA, respectively. Also note the symmetry of the Doppler spectral waveform when comparing flow towards the transducer (positive) with flow away from the transducer (negative).
Figure 6 shows sample spectra and M-mode images from different time points in the breath-hold maneuver. Figure 6A shows the baseline TCD spectrum and M-mode at the beginning of breath-holding. Note the mean velocity of 56 cm/s. Figure 6B shows the TCD spectrum and M-mode at the end of breath-holding. Note that the mean velocity has now increased to 70 cm/s. Figure 6C shows the TCD spectrum and M-mode after the end of breath-holding. Note the undershoot in velocity below baseline values, with the mean dropping to 47 cm/s. Note that the ACA is visible as flow away from the transducer in the Doppler spectra.
Figure 7 shows the entire breath-holding experiment. Note that the envelope remains elevated for approximately 15 s after breath-holding ends, falls to values lower than those at the beginning of breath-holding for ~20 s, and then finally recovers to baseline values. Note that the ACA is visible as flow away from the transducer in the Doppler spectrum.
Figure 6 and Figure 7 display good signal intensity in the MCA portion of the TCD spectrum (the MCA is represented by the positive velocities); note how the white line which represents the envelope follows the TCD spectrum very accurately when the spectrum is bright. The spectra of Figure 6 and Figure 7 could be improved by decreasing the monitoring depth by 5–10 mm so that the ACA portion of the TCD spectrum would not be visible (the ACA is represented by negative velocities) and by changing the scale of the vertical axis in the TCD spectrum to run from approximately -100 cm/s to 100 cm/s, which would allow maximum velocity sampling of the TCD spectrum in the vertical direction.
Figure 8 shows examples of bilateral TCD spectra and M-modes suitable for bilateral fTCD. Figure 8A and Figure 8B demonstrate acceptable, but not optimal, bilateral spectra and M-modes. Note how the gain is higher in Figure 8A (left MCA) than in Figure 8B (right MCA) to compensate for the weaker signal, and how the envelope quality in Figure 8A is slightly poorer than in Figure 8B. Also note how the maximum velocity at systole in Figure 8A is slightly lower than in Figure 8B. By contrast, note how the two spectra in Figure 8C and Figure 8D are very similar in terms of settings, including depth, gain, power, and sample volume, and how the spectral waveforms on both sides have similar maximum velocities and shapes. To address this, it is recommended that the spectrum from the left MCA be consistently placed in the left window and the spectrum from the right MCA in the right window, especially for experiments involving lateralization of blood flow.
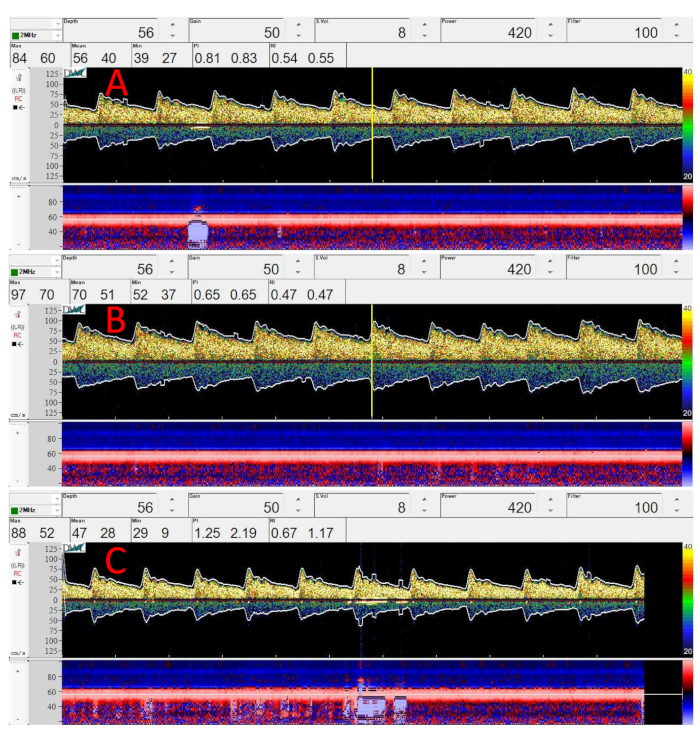
Figure 6: Sample Doppler spectra and M-mode images from the MCA during different stages of the breath-hold maneuver. (A) Spectrum and M-mode at the beginning of breath-holding. Vertical yellow line in center denotes the start of breath-holding. (B) Spectrum and M-mode at the end of breath-holding. Vertical yellow line in center denotes the end of breath-holding when the subject inhales. (C) Spectrum and M-mode after the end of breath-holding, showing the decrease in flow velocity that persists for approximately 30 s after breath-holding. In all spectra, depth = 56 mm, gain = 50, sample volume = 8 mm, power = 420 mW/cm2, and filter = 100 Hz. Please click here to view a larger version of this figure.
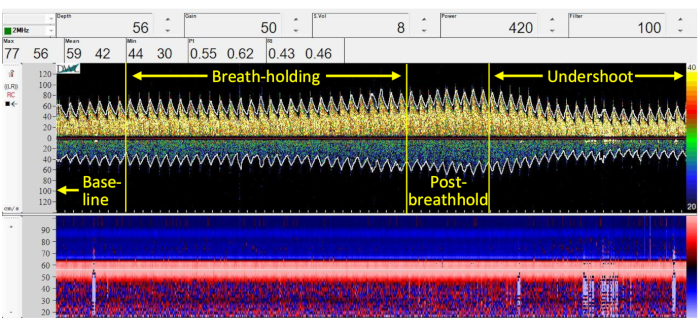
Figure 7: Spectrum and M-mode from the MCA throughout breath-holding. Depth = 56 mm, gain = 50, sample volume = 8 mm, power = 420 mW/cm2, and filter = 100 Hz. Please click here to view a larger version of this figure.
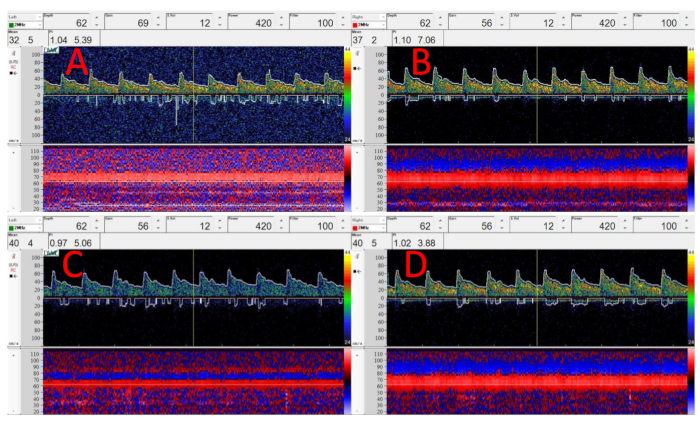
Figure 8: Examples of bilateral spectra and M-mode images from the MCA. (A) Acceptable, but not optimal, spectrum and M-mode of the left MCA, with depth = 62 mm, gain = 69, sample volume = 12 mm, power = 420 mW/cm2, and filter = 100 Hz. (B) Good spectrum and M-mode of right MCA, with depth = 62 mm, gain = 56, sample volume = 12 mm, power = 420 mW/cm2, and filter = 100 Hz. (C) Good spectrum and M-mode of the left MCA. (D) Good spectrum and M-mode of the right MCA. For both (C) and (D), depth = 62 mm, gain = 56, sample volume = 12, power = 420 mW/cm2, and filter = 100 Hz. Please click here to view a larger version of this figure.
| Age | Middle cerebral artery depth (mm) |
| 0–3 monthsa | 25 |
| 3–12 monthsa | 30 |
| 1–3 yearsa | 35–45 |
| 3–6 yearsa | 40–45 |
| 6–10 yearsa | 45–50 |
| 10–18 yearsa | 45–50 |
| >18 yearsb | 50 |
Table 1: MCA depths at various ages. Sources: a = Bode25, b = Alexandrov et al.10
