El shock cardiogénico (SC) es un estado de hipoperfusión tisular con o sin hipotensión concomitante, en el que el corazón no puede suministrar suficiente sangre y oxígeno para satisfacer las demandas del cuerpo, lo que resulta en insuficiencia orgánica. Se clasifica en estadios A a E por la Society of Cardiovascular Angiography and Interventions (SCAI): estadio A – pacientes en riesgo de SC; estadio B – pacientes en la etapa inicial de CS con hipotensión o taquicardia sin hipoperfusión; estadio C – SC clásico con fenotipo frío y húmedo que requiere inotropos/vasopresores o soporte mecánico para mantener la perfusión; etapa D: deterioro en el soporte médico o mecánico actual que requiere escalamiento a dispositivos más avanzados; y estadio E: incluye pacientes con colapso circulatorio y arritmias refractarias que están experimentando activamente un paro cardíaco con reanimación cardiopulmonar en curso1. Las causas más comunes de SC son el IM agudo (IAM), que representa el 81% de los casos en un análisis notificado recientemente2, y la insuficiencia cardíaca aguda descompensada (ADHF). El SC se caracteriza clásicamente por congestión y alteración de la perfusión, que se manifiesta por presiones de llenado elevadas (presión de cuña capilar pulmonar [PCWP], presión diastólica final del ventrículo izquierdo [LVEDP], presión venosa central [CVP] y presión diastólica final del ventrículo derecho [RVEDP]), disminución del gasto cardíaco (CO), índice cardíaco (IC), gasto de potencia cardíaca (CPO) y mal funcionamiento del órgano final3 . En el pasado, los únicos tratamientos disponibles para el IAM complicado por SC eran la revascularización temprana y el tratamiento médico con inotropos y/o vasopresores4. Más recientemente, con el advenimiento de los dispositivos de soporte circulatorio mecánico (SQM) y el reconocimiento de que la escalada de vasopresores se asocia con un aumento de la mortalidad, se ha producido un cambio de paradigma en el tratamiento de la CS5 relacionada con el IAM y la ADHF5,6.
En la era actual de los dispositivos de asistencia ventricular percutánea (pVAD), hay una serie de plataformas/configuraciones de dispositivos MCS disponibles, que proporcionan soporte circulatorio y ventricular univentricular o biventricular con y sin capacidad de oxigenación7. A pesar de los aumentos constantes en el uso de pVAD para tratar tanto el IAM como el SC ADHF, las tasas de mortalidad se han mantenido en gran medida sin cambios5. Con la evidencia emergente de posibles beneficios clínicos para la descarga temprana del ventrículo izquierdo (VI) en AMI8 y el uso temprano de MCS en AMI CS9, el uso de MCS continúa aumentando.
El dispositivo MCS de derivación de la arteria auricular izquierda a femoral (LAFAB) evita el VI drenando la sangre de la aurícula izquierda (LA) y devolviéndola a la circulación arterial sistémica a través de la arteria femoral (Figura 1). Está soportado por una bomba centrífuga externa que ofrece un flujo de 2.5-5.0 litros por minuto (L / m) (bomba de nueva generación, designada como LifeSPARC, capaz de hasta 8 L / m de flujo) dependiendo del tamaño de las cánulas. Una vez que la sangre se extrae de la LA a través de la cánula venosa transseptal, pasa a través de la bomba centrífuga externa que recircula la sangre de nuevo en el cuerpo del paciente a través de la cánula arterial colocada en la arteria femoral.
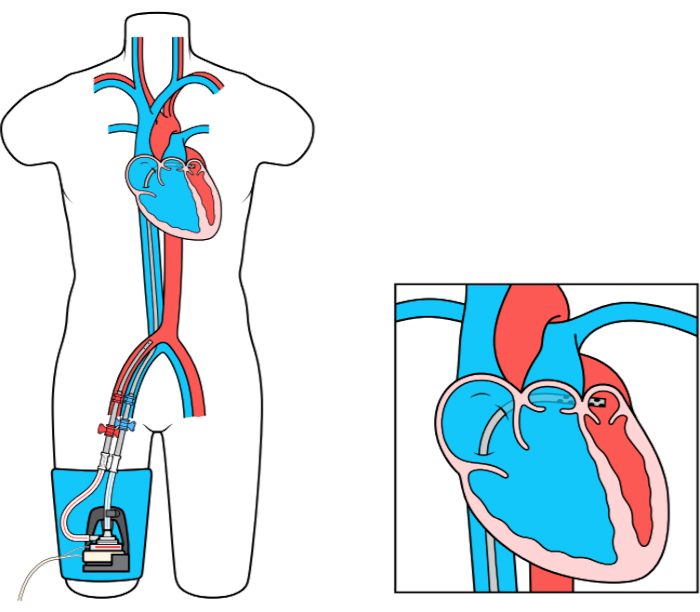
Figura 1: Configuración de LAFAB. Imagen cortesía de TandemLife, una subsidiaria de propiedad total de LivaNova US Inc. Haga clic aquí para ver una versión más grande de esta figura.
