All the animal procedures performed were approved by the institutional animal ethical committee of JSS College of Pharmacy, Ooty, India.
1. Preparation of DOX loaded porous scaffolds by freeze-drying method
- Add 1.2 g of COL to 100 mL of water (e.g., Millipore) and keep aside for swelling.
- Stir the swollen COL dispersion at 2000 rpm overnight to ensure complete dissolution of COL.
- Prepare CS solution by dissolving approximately 0.8 g of CS in 100 mL of 1% acetic acid.
- Stir the CS solution overnight at 2000 rpm to ensure uniform dispersion.
- Mix DOX (1% w/v), followed by CS solution, to the COL solution, and stir for 30 min.
- Filter the obtained physical mixture using a muslin cloth to remove the particulate matter.
- Deep freeze the obtained filtrate at -85 °C ± 4 °C for about 24 h.
- Lyophilize the deep freeze mixture at -85 °C ± 4 °C for 72 h.
- Store the obtained scaffolds in a desiccator for further analysis 16,17.
2. Crosslinking of scaffold
- Dissolve MES (0.488 g) in 50 mL of water.
- Soak 50 mg of the DOX loaded scaffold in 20 mL of the MES buffer for 30 min.
- Mix 19.5 mL of MES buffer with 0.1264 g of EDC and 0.014 g of NHS in a separate beaker.
- Immerse the scaffold in the buffer mixture for 4 h to achieve crosslinking 16.
- Store the DOX loaded crosslinked (CL) and non-crosslinked scaffolds (NCL) for further evaluation.
3. Characterization of scaffolds
- Morphological examination using a scanning electron microscopy (SEM)
- Characterize the scaffolds for morphological analysis using SEM (1 cm × 1 cm × 0.5 cm).
- Stain the cross-section and exterior surface of the scaffold with the delicate layer of gold (~150 Å).
- Capture the photographic image at the excitation voltage of 5 kV and 10 kV.
- Place the samples in aluminum stubs and enclose them with the gold at approximately 9 V.
- Measure the scaffold using SEM with the increased resolution at 10 kV.
- Porosity determination
- Measure the porosity of the scaffolds using the liquid displacement method (ethanol) 18.
- Calculate the porosity of the scaffolds using the below formulae.

Ww = Wet weight of the scaffold
Wd = Dry weight of the scaffold
Wv = Volume of the scaffold
- Determining the water absorption capacity
- Measure the dry weight of the scaffold.
- Incubate the weighed scaffold at 37 °C for 24 h in phosphate buffer saline (PBS) pH 7.4.
- Remove the excess PBS over the scaffold using filter paper.
- Measure the water absorption capacity using the below formulae 17.

WS = Percentage of water absorption
W1=Wet weight of the scaffold
W0= Dry weight of the scaffold
- Scaffold degradation
- Incubate the scaffold (1cm x 1cm) at 37 °C for 7 days in a PBS of pH 7.4 containing lysozymes.
- Wash the scaffold to remove any adhered ions on the surface.
- Freeze dry the washed scaffold 17.
- Calculate the rate of degradation using formulae.

Ww = Initial weight of the scaffold
Wd = Weight of the scaffold after freeze-drying
- In vitro release studies
- Determine the release behavior of the DOX from the scaffold using the dialysis sack method.
- Disperse the scaffold in a few milliliters of simulated wound fluid (pH 7.4) and transfer it into a dialysis bag.
- Tightly close the ends of the membrane bag and immerse in the 500 mL of simulated wound fluid solution.
- Stir the wound fluid solution containing the dialysis bag at 200-250 rpm.
- Collect the supernatant solution and replace it with an equal quantity of fresh buffer solution at definite time intervals.
- Determine the percentage of DOX release from the scaffolds in the supernatant solution using a UV-visible spectrometer at 240 nm.
4. In vitro anti-bacterial studies
- Determine the minimum inhibitory concentration (MIC) of the CL and DOX-CL scaffolds against the S. aureus, S. epidermis, E. coli, P. aeruginosa using the micro-broth dilution method.
- Prepare the bacterial cultures using Mueller-Hinton broth at a ratio of 1:1000 to obtain 0.5 McFarland turbidity.
- Add D-glucose (800 mg/dL) to the bacterial cultures for hyperglycation 19,20.
- Mince and solubilize the CL and DOX-CL in DMSO (negative control).
- Serially dilute the hyperglycated bacterial suspension (100 µL) and test samples (100 µL of scaffolds solution) in 96 well plate.
- Incubate the plate at 37 °C for 20-24 h.
- Record the absorbance at a wavelength of 600 nm 21.
5. In vitro biocompatibility studies
- Evaluate the biocompatibility of the prepared scaffolds using MTT [(3-(4, 5 dimethyl thiazole-2 yl) -2, 5-diphenyl tetrazolium bromide)] assay.
- Sterilize the scaffolds of standard dimension and place them in 24 well plates.
- Add 3T3-L1 cells to the 24 well plate and incubated for 72 h.
6. In vivo animal studies
- Induction of DM and excision wound
- Feed the animal with a high-fat diet for two weeks and administer a single dose of streptozotocin (STZ) (50 mg/kg body weight) in citrate buffer solution intraperitoneally to Wistar albino rats (180-200 g) for the induction of type-2 diabetes.
- Choose the animals with a constant blood glucose of 250 mg/dL for the study.
- Randomize the selected animals for the induction of excision wounds.
- Anesthetize the diabetic rats using diethyl ether (5 mL was added to the priorly saturated anesthesia chamber) and confirm using the toe pinch method and mucous membrane color.
- Shave the dorsal area (Dorsal thoracic, lumbar region) using an aseptic trimmer and blades (A40).
- Sterilize the shaved area with an alcoholic swab.
- Excise the skin (2 x 2 cm2 and a depth of 1 mm) with an aseptic surgical A40 blade on the shaved area to create an open wound.
- Divide the animals into three groups (Group 1- Disease control (Control), Group 2- CL scaffold (Placebo), Group 3- DOX CL scaffold), each group consisting of 6 rats.
- Affix the CL and DOX CL scaffolds using surgical tape and cover the control group with sterile gauze for 21 days.
- Trace the wound area on a sterile OHP sheet and measure the percentage reduction of the wound using the grid method on days 0, 7, 14, and 21 for all groups.
- Calculate the percentage wound reduction using the below formulae.

7. Histopathological studies
- Isolate the healed wound area on days 7, 14, and 21, store in formalin solution (10%).
- Section the tissues using a microtome to obtain a thickness of 6 µm.
- Mount the sections on a glass slide and stain using Hematoxylin and eosin 17.
- Capture the images under 40x magnification using a digital microscope.
8. Hydroxyproline estimation
- Isolate the healed wound area on days 0, 7, 14, and 21 for evaluation.
- Estimate the hydroxyproline content using the procedure described by Reddy G et al., 1996 22.
9. Elisa test
- Estimate the MMP-9 levels using the Elisa kit as per the manufacturer's instructions.
- Isolate the tissue samples from the healed wound area on day 21 and mince using a tissue homogenizer.
- Centrifuge the obtained homogenate and collect the supernatant.
- Dilute the supernatant at 100-fold using assay buffer.
- Scan the plate using a multiple plate reader.
10. Statistical analysis
- Represent the obtained outcomes as Mean ± SD.
- Perform the statistical analysis using Graph pad prism v5.01.
- Attain the statistical significance using One Way Analysis of Variance (ANOVA) and Dunnet's post hoc test.
- Consider the values with p≤0.05 as significant.
Characterization of the DOX loaded NCL and CL scaffold
On visual examination, the NCL and CL scaffold was found to be cream in color. Besides, both the scaffolds appear to be like a sponge, stiff and inelastic when examined physically. SEM images of the NCL and CL scaffolds are shown in Figure 1. From the figure, it was clear that there was a decrease in pore size after crosslinking by forming intermolecular linkages. Also, the NCL and CL scaffolds porosity were found to be 92.3±4.21 and 71.35±2.65, respectively. The percentage of water absorption of the NCL and CL scaffolds was 750±11.4% and 492±8.66% at 24 h time intervals.
In addition, biodegradation studies were performed for seven days in the simulated wound fluid of pH 7.4, comprising lysozymes. The NCL scaffold exhibited a faster rate of degradation initially in the first three days and decreased slowly for four consecutive days. On the other side, the CL scaffold showed a prolonged rate of degradation. Crosslinking of the scaffold enhanced mechanical properties and network strength that, in turn, resulted in decreased degradation rate, indicating improved resistance to the degradation (Figure 2).
Further, the in vitro release of DOX from NCL and CL scaffold was performed for 120 h (Figure 3). In the initial 1 h, 27.92±3.45% DOX was released from the NCL scaffold, whereas only 16.54±2.21% DOX was released from the CL scaffold. After 6 h, the DOX release from the scaffolds increased by 63.15±3.78% in the NCL scaffold and 44.43±3.57% in CL scaffolds. After 24 h, there was a release of 70% DOX from the NCL scaffold, whereas CL scaffold took more than 72 h to release 70% of the DOX. Based on the results obtained, the DOX loaded CL scaffold was selected for further evaluation and represented as DOX-CL scaffold. Whereas CL scaffold without DOX (placebo) is designated as CL Scaffold.
In vitro anti-bacterial studies
Patients with DW usually experience infections that result in prolonged wound healing. Thus, prepared scaffolds were examined for their anti-bacterial activity using the MIC against a selected panel of bacteria (Table 1). From the results, it is clear that DOX exhibited inhibitory activity with a MIC of <4 µg/mL against both S. aureus and S. epidermis. A MIC of <8 µg/mL and <16 µg/mL was observed against E. coli and P. aeruginosa. Alone chitosan and CL scaffold extract exhibited minimal activity against selected organisms such as S. aureus (<64 µg/mL), S. epidermis (<64 µg/mL), E. coli (<128 µg/mL), and P. aeruginosa (<128 µg/mL). DOX-CL scaffold has shown similar inhibitory activity with a MIC of <2 µg/mL against both S. aureus and S. epidermis. Further, the DOX-CL scaffold exhibited moderate activities with a MIC of <8 µg/mL against E. coli and P. aeruginosa.
In vitro biocompatibility study
MTT assay was performed to determine the cellular viability of 3T3-L1 cells in the presence of CL and DOX-CL scaffolds. The results exemplified that the CL and DOX-CL scaffolds did not stimulate any cytotoxicity. Furthermore, the cellular viability was comparatively higher in the scaffold treated groups than in control, representing the enhanced growth of fibroblasts in the presence of scaffolds (Figure 4).
In vivo wound healing studies
The mean wound area decreased in all the groups was determined using the graphical method on days 0, 7, 14, and 21 (Figure 5). On visual examination, the wounds in the CL and DOX-CL scaffold treated groups were free from oozing on day seventh. At the same time, the wounds in the control group were oozing. On day 14, a dry scab was observed in all groups; however, a faster rate of wound contraction was observed in the DOX-CL scaffold (89.663%). On day 21, 99.9% of the wound got healed, and a scar was formed in the DOX-CL scaffold, whereas partial healing was observed in control and CL scaffold treated groups.
Histopathology study
Histopathological observation of wound healing on day seventh postinjury exhibited disruption of all skin layers at the edges of the wound in all groups. There was no visibility of the epidermis; however, predominant neutrophils with intermittent monocytes and lymphocytes were observed in the control group. In CL scaffold treated group, moderate visibility of epidermis was noticed along with few neutrophils and macrophages. Whereas, in the DOX-CL scaffold treated group, the wound was covered with a slim layer of the epidermis, representing the phase of reepithelization. Mild neutrophils and macrophages, along with granulation tissue, were also seen more often in the DOX-CL scaffold treated group.
On day 14 postinjury, wounds in all the groups were found to be covered with epidermis. In the control group, the epidermis layer formed was observed to be a very slim layer along with prevailed neutrophils. In the CL scaffold treated group, the epidermis layer formed was thicker than that in the control group, along with mild multinucleated massive cells. In the DOX-CL scaffold treated group, the epidermis developed was thicker compared to other groups, along with an abundant number of histiocytes and giant multinucleated cells. The dense zone of fibroblasts was also observed in the DOX-CL scaffold treated group.
On day 21 postinjury, in the control group, a dominant number of neutrophils were decreased along with recurrence of macrophages and histiocytes representing the decreased inflammation. Whereas, in the CL scaffold treated group, a moderate number of histocytes and lymphocytes were observed. The epidermis formed was observed to be substantially thicker in the DOX-CL scaffold treated group than those in the control group, along with a rich number of histiocytes, lymphocytes, and massive multinucleated cells. In the DOX-CL scaffold treated group, the neutrophils count was decreased on day 7. Also, the gathering of macrophages and their morphological variants such as multinucleated massive cells and histiocytes were noticed on day 14 and 21 (Figure 6).
Hydroxyproline estimation
Hydroxyproline estimation is an indirect measure of the amount of collagen present in healing wounds. Higher hydroxyproline concentration designates a rapid percentage of wound healing. The biochemical examination revealed a higher amount of hydroxyproline in the DOX-CL scaffold treated group followed by the CL scaffold treated group than those in the control group (Figure 7).
MMP-9 estimation using the Elisa kit
MMP-9 content in the DOX-CL scaffold treated group was significantly decreased compared to those in control, and CL scaffold treated group. Whereas the MMP-9 content in the CL scaffold treated group was marginally less compared with that of the DOX-CL scaffold treated group, as shown in Figure 8.
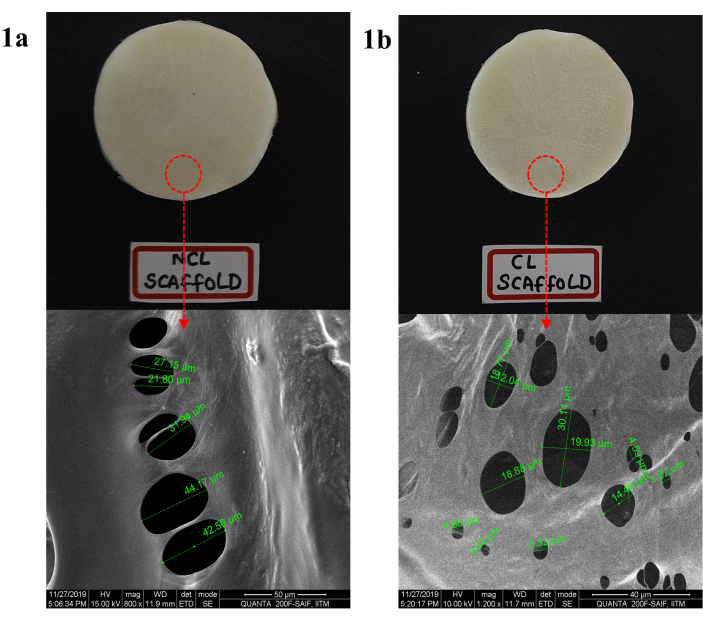
Figure 1: Morphology of DOX loaded COL-CS scaffold a) before CL and b) after CL determination by SEM at a scale range of 50 µm. Please click here to view a larger version of this figure.
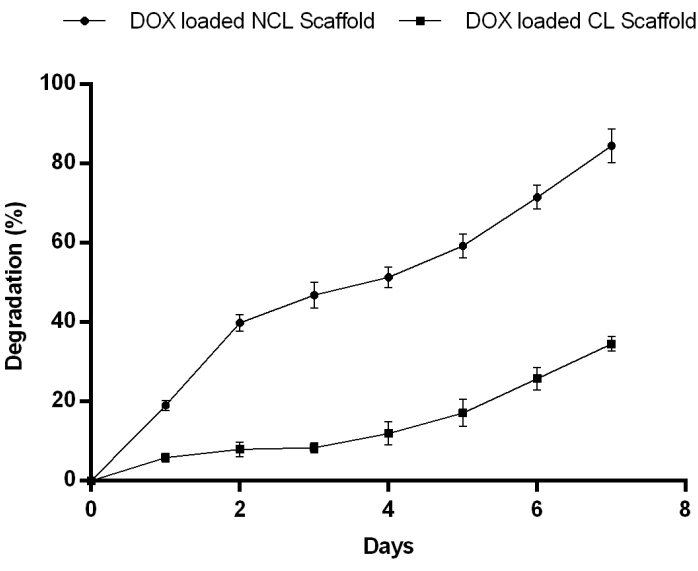
Figure 2: Matrix degradation of DOX loaded in NCL and CL scaffolds from day 1 to 7 in PBS pH 7.4 at 37 °C showing NCL degraded gradually for 7 days. Contrary to this, the CL scaffold degradation rate reduced considerably indicates enhanced resistance to enzymatic degradation. Please click here to view a larger version of this figure.
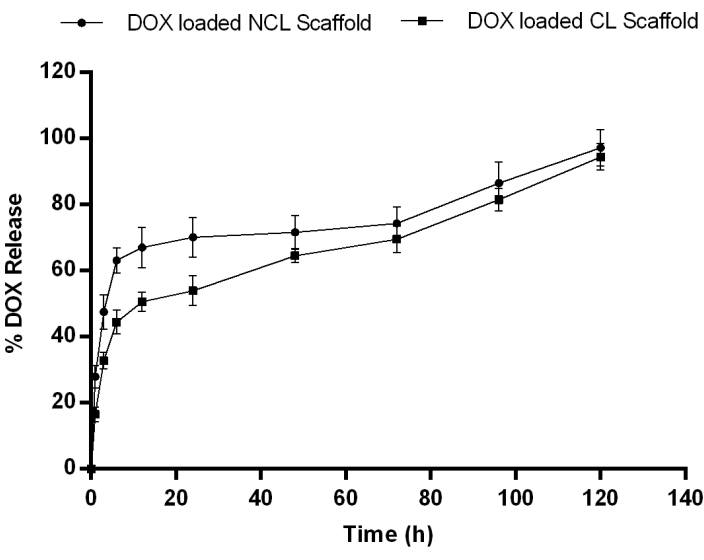
Figure 3: In vitro drug release profile of DOX from NCL and CL scaffolds in PBS pH 7.4 at 37° C showing a slow release of drug in all formulation followed by a sustained release. Data expressed as mean ± SD (n=3). Please click here to view a larger version of this figure.
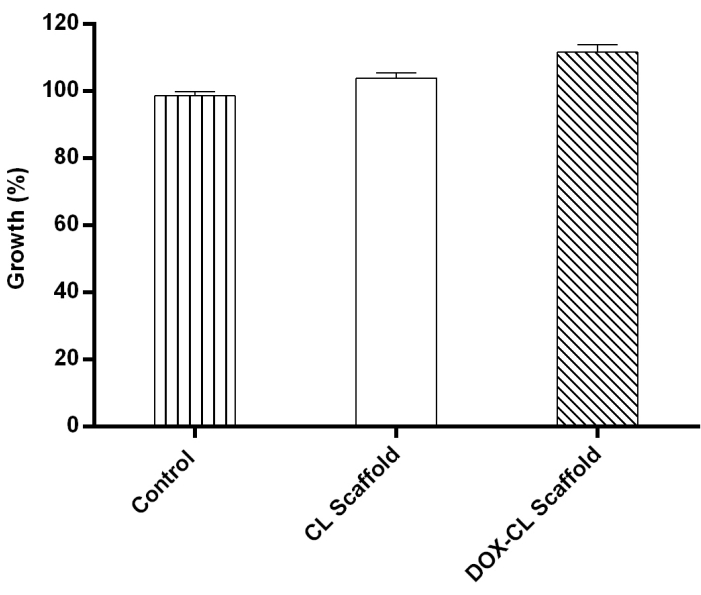
Figure 4: 3T3-L1 cells cultured in the presence of CL and DOX-CL scaffolds showing percentage cell growth more in DOX-CL scaffold treated group followed by CL scaffold treated and control. Please click here to view a larger version of this figure.
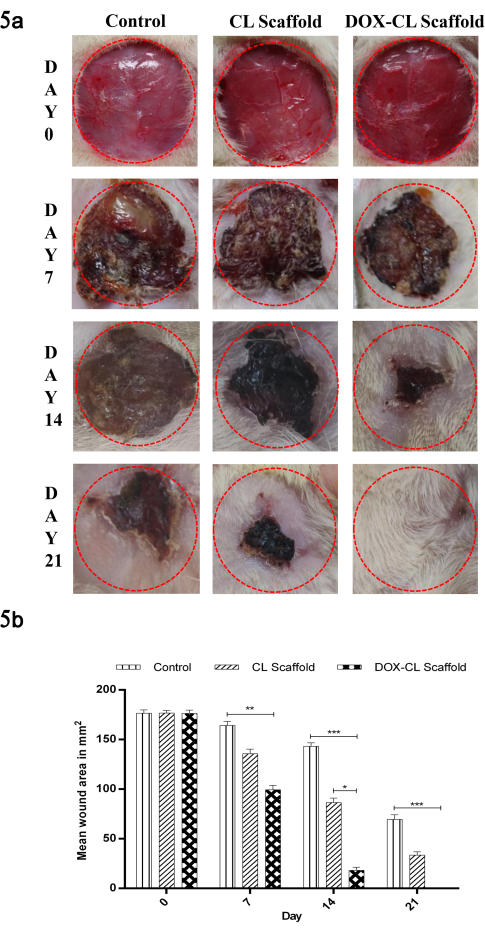
Figure 5: (a) Images representing the reduction in mean wound area in the control, CL scaffold and DOX-CL scaffold treated groups on day 0, 7, 14 and 21 post wounding. (b) Graphical representation of reduction in mean wound area in the control, CL scaffold and DOX-CL scaffold treated groups on day 0, 7, 14 and 21 post wounding. Data is expressed as mean ± SD (n=6 wounds/ group). Statistical significance was obtained by One Way Analysis of Variance (ANOVA) followed by Dunnet's post hoc test. Please click here to view a larger version of this figure.
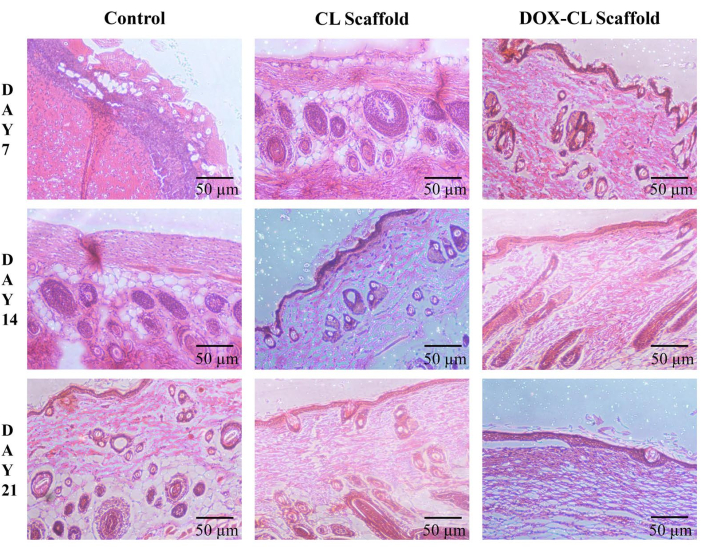
Figure 6: Histological changes during the wound healing process in STZ and high-fat diet-induced induced diabetes in Wistar albino rat skin on days 7, 14, and 21 without (control) and with treatment (CL and DOX-CL scaffolds) in a full-thickness excision wound model. Please click here to view a larger version of this figure.
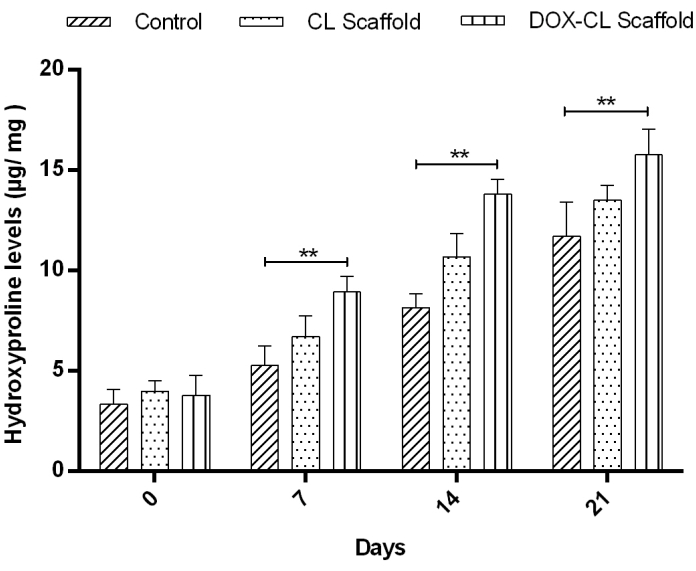
Figure 7: Result representing the hydroxyproline content in wounds on days 0, 7, 14, and 21 as an indicator of indirect collagen level estimation. The results are expressed in µg hydroxyproline/ mg of dry wound tissue. The data represents the Mean±SD (n=6 wounds/group). Statistical significance was obtained by One Way Analysis of Variance (ANOVA) followed by Dunnet's post hoc test. Please click here to view a larger version of this figure.
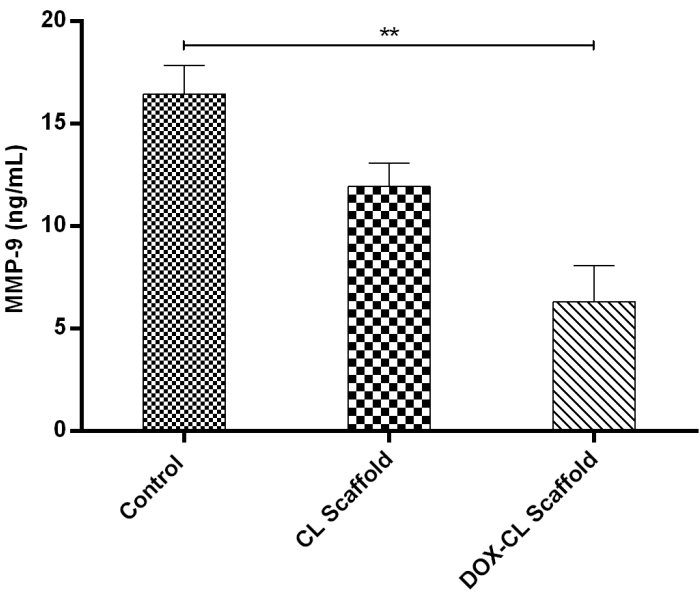
Figure 8: Graph representing the MMP-9 levels in homogenates obtained from healed wounds in STZ and high-fat diet-induced induced diabetic rat model on day 21. Levels of MMP-9 were determined in 100-fold aliquots of wound fluids using ELISA analysis. The data represent Mean±SD (n=3). Please click here to view a larger version of this figure.
| MIC (µg/mL) | ||||
| Test sample | S. aureus | S. epidermis | E. coli | P. aeruginosa |
| DOX | <4 | <4 | <8 | <16 |
| CS | <64 | <64 | <128 | <128 |
| CL scaffold extract | <64 | <64 | <128 | <128 |
| DOX-CL scaffold extract | <2 | <2 | <4 | <4 |
Table 1: Minimum inhibitory concentration of CS, DOX, CL, and DOX-CL Scaffolds against a selected panel of bacteria.
