The PaO2/FIO2-ratio decreased during surfactant washout in all animals (Figure 3). The resulting hypoxemia, hypercapnia, and atelectasis caused an increase in pulmonary artery pressure. The details of the lung lavages are already described elsewhere6.
The surfactant depletion was repeated until the PaO2/FIO2 ratio remained below 100 mmHg despite mechanical ventilation with a PEEP of 5 mbar for at least 5 min. Afterwards, ventilation with high tidal volumes, low PEEP, and nearly complete inflation/deflation was commenced for 2 h to cause VILI. Of note, parameters of gas exchange (oxygen saturation, PaO2) can improve during ventilation with high tidal volumes due to the cyclic recruitment while mPAP usually remains elevated due to high intrathoracic pressures and hypercapnia (Figure 3B). On average, induction of anesthesia, instrumentation, surfactant depletion, and injurious ventilation require about 5 h depending on experience of the investigator and the number of lavages required to achieve the targeted PaO2/FIO2 ratio.
The recruitability of the lungs was tested after each experimental step with a recruitment maneuver (inspiratory pressure of 50 mbar and PEEP 24 mbar for five breaths). An arterial blood gas sample was taken 5 min after the recruitment maneuver while ventilation was commenced with a tidal volume of 6 mL/kg bw, a PEEP of 15 mbar and an FIO2 of 1.0. This recruitment maneuver resulted in a notable increase in the oxygenation in all the animals after surfactant washout (Figure 3a), whereas 2 h of injurious ventilation diminished lung recruitability with respect to gas exchange and mPAP (Figure 3, Table 1). The lung injury induced with the protocol was not prone to recruitment even when ventilation was performed according to the ARDS-Network high PEEP table for 3 h after an additional recruitment maneuver.
Computer tomographic (CT) imaging of one animal showed atelectasis of the dependent areas of the lung during ventilation with a PEEP of 6 mbar, which resolved largely when ventilation was escalated to a PEEP of 15 mbar (Figure 4), whereas the substantial ubiquitous ground glass opacities did not resolve. Furthermore, some CT findings such as alveolar opacities indicated structural damage of the lungs corresponding with post-mortem examination of the lungs (Figure 4).
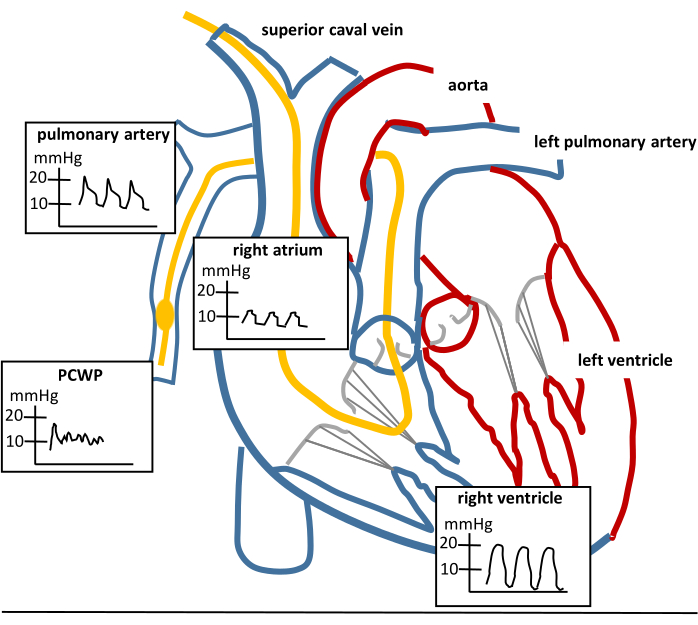
Figure 1: Pulmonary artery catheter placement. Sketch of the heart, a properly placed pulmonary artery catheter (PAC; yellow catheter) and the respective waveforms that can be seen while advancing a PAC. PCWP means pulmonary capillary wedge pressure. The PCWP waveform can only be seen in wedge position while the balloon is inflated. The PCWP curve should disappear and the pulmonary artery curve should be visible if the balloon is deflated and the PAC is placed properly. Please click here to view a larger version of this figure.
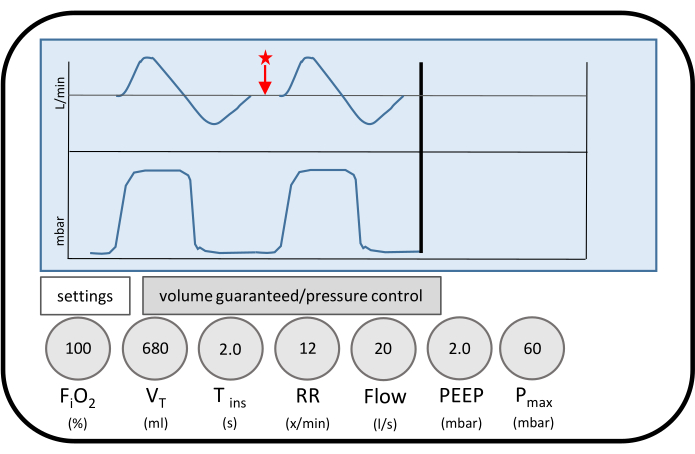
Figure 2: Ventilator settings of injurious ventilation. Displayed are the ventilator settings during ventilation to provoke ventilator-induced lung injury (VILI). The tidal volume corresponds to 17 mL/kg body weight in the respective animal. The flow pattern decreases to zero flow on expiration (red star). Zero flow is maintained for a relevant period of the respiratory cycle. Thus, almost complete inflation and deflation of the lungs is achieved to promote baro- and atelectrauma. Please click here to view a larger version of this figure.
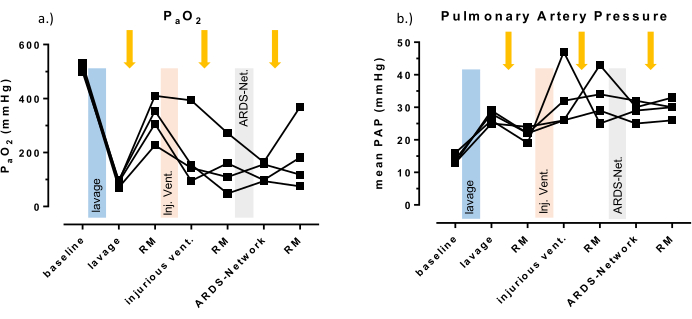
Figure 3: Systemic oxygenation and pulmonary artery pressure. (A) Individual results of the partial arterial pressure of oxygen. (B) Mean pulmonary arterial pressure of four animals are displayed as representative values for the induced lung injury. Test for statistical significance were not performed due to the small number of animals (n = 4). A recruitment maneuver was performed after each intervention (yellow arrows) to test for recruitability of the model. Note that PaO2 increases after lung lavage and after recruitment by at least 150 mmHg, but not after injurious ventilation. Please click here to view a larger version of this figure.
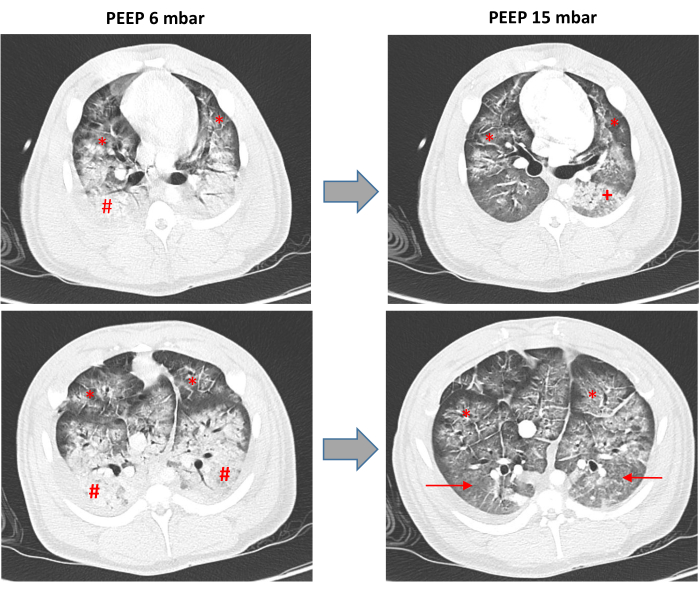
Figure 4: Computed tomography of the lungs. Representative computer tomographic scans (CT) of one animal after surfactant washout and mechanical ventilation with high tidal volumes and low PEEP to cause ventilator-induced lung injury (VILI). The scans were taken during ventilation with high positive end expiratory pressure of 15 mbar (PEEP 15 mbar) and low PEEP of 6 mbar (PEEP 6 mbar) with a tidal volume of 6 mL/kg body weight. The upper panels show the same apical region of the lungs. The lower panels show the same region of the lung at height of the heart. The # marks the dependent lung areas with basal atelectasis; the → marks the dependent lung areas/former atelectasis, which are recruited under ventilation with a PEEP of 15 mbar; the * marks extensive ground glass opacities with superimposed inter- and intralobular septeal thickening, which are not resolved during ventilation with a PEEP of 15 mbar, the + marks diffuse alveolar opacifications, which indicate alveolar hemorrhage and are not visible during ventilation with a PEEP of 6 mbar due to the extensive atelectasis. Please click here to view a larger version of this figure.
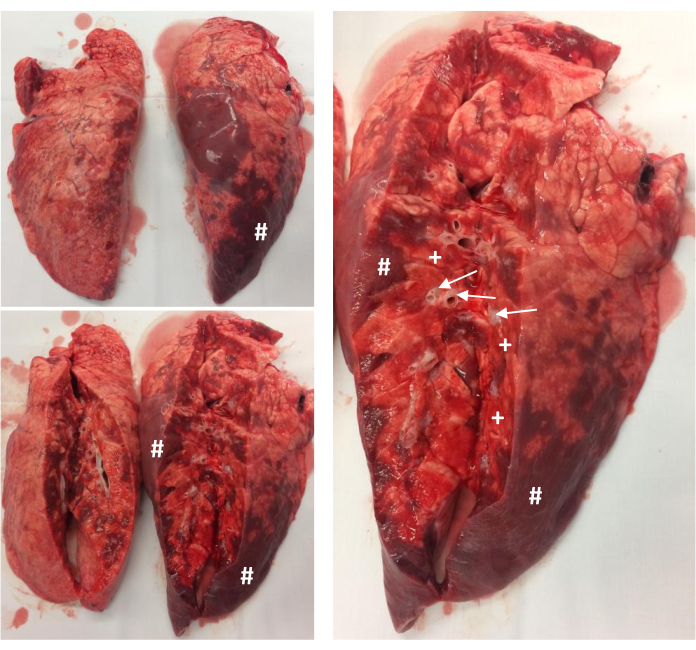
Figure 5: Postmortem examination of the lungs. Representative pathology of the unfixed lungs of one animal right after the experiment. The basal area of the lungs faces toward the reader. The # marks atelectasis; the + marks diffuse alveolar hemorrhage; the → marks distended, edematous peribronchial spaces. Please click here to view a larger version of this figure.
| baseline | after lavage | RM | after injuriuos ventilation | RM | after ARDS-Net | RM | |
| PaO2 (mmHg) |
514 ±13 |
87 ±12 |
324 ±78 |
197 ±134 |
147 ±95 |
128 ±37 |
185 ±129 |
| PaCO2 (mmHg) |
48 ±6 |
86 ±10 |
82 ±12 |
66 ±5 |
96 ±4 |
92 ±5 |
123 ±10 |
| pH | 7.39 ±0.09 |
7.14 ±0.05 |
7.17 ±0.08 |
7.26 ±0.06 |
7.11 ±0.04 |
7.14 ±0.04 |
7.04 ±0.03 |
| lactate (mg/dL) |
4 ±3.9 |
6 ±5.0 |
6 ±5.9 |
4 ±3.6 |
4 ±3.5 |
4 ±3.6 |
6 ±5.3 |
| heart rate (beats/min) |
86 ±8 |
90 ±11 |
92 ±12 |
104 ±18 |
129 ±30 |
147 ±13 |
149 ±5 |
| CO (L/min) | 4 ±0.8 |
3.7 ±1.4 |
3.6 ±0.8 |
5.2 ±0.8 |
5.1 ±0.8 |
6.9 ±1.0 |
|
| mAP (mmHg) |
93 ±4 |
101 ±21 |
108 ±31 |
78 ±8 |
96 ±31 |
65 ±12 |
72 ±9 |
| SVR (dyn.sec.cm-5) |
1856 ±302 |
2552 ±777 |
1624 ±468 |
1179 ±237 |
903 ±292 |
711 ±166 |
|
| mPAP (mmHg) |
14 ±1 |
27 ±2 |
22 ±2 |
33 ±10 |
33 ±8 |
29 ±3 |
30 ±3 |
| PVR (dyn.sec.cm-5) |
106 ±170 |
267 ±442 |
170 ±258 |
92 ±126 |
108 ±160 |
66 ±88 |
|
| PCWP | 6 ±2 |
10 ±2 |
8 ±2 |
9 ±1 |
10 ±4 |
11 ±5 |
|
| Cdyn (mL/mbar) |
33 ±4 |
12 ±2 |
21 ±4 |
23 ±8 |
20 ±2 |
26 ±8 |
24 ±5 |
Table 1: Arterial blood gases, hemodynamic data and lung compliance. The table presents the respective arterial blood gases and hemodynamic data. RM: recruitment maneuver, PaO2: arterial partial pressure of oxygen, PaCO2: arterial partial pressure of carbon dioxide, CO: cardiac output, MAP: mean arterial pressure, SRV: systemic vascular resistance, mPAP: mean pulmonary arterial pressure, PVR: pulmonary vascular resistance, PCWP: pulmonary capillary wedge pressure. Data presented as mean ± SD.
| baseline | after lavage | RM | ||||||
| I | PaO2 (mmHg) | 540 | 81.3 | 270 | 21.9 | -the recruitment maneuver after surfactant depletion was preformed without prior injection of a muscle relaxant -the recruitment maneuver (RM) resulted in a tension pneumothorax with rapid cardiopulmonary deterioration (grey background) despite immediate chest drain insertion – following animals received a bolus injection of a muscle relaxant prior to a RM and the problem was not observed again |
||
| PaCO2 (mmHg) | 42.6 | 69.4 | 84.9 | 93.9 | ||||
| pH | 7.44 | 7.17 | 7.01 | 6.99 | ||||
| Lactate (mmol/L) | 11 | 17 | 67 | 56 | ||||
| heart rate (beats/min) | 138 | 155 | 141 | 221 | ||||
| CO (L/min) | 7.7 | 3.6 | 1.6 | |||||
| mAP (mmHg) | 82 | 60 | 143 | 53 | ||||
| mPAP (mmHg) | 26 | 18 | 22 | 22 | ||||
| PCWP (mmHg) | 10 | 12 | 12 | 17 | ||||
| Cdyn (mbar/mL) | 35 | 11 | 19 | 13 | ||||
| PCWP (mmHg) |
10 | 12 | 12 | 17 | ||||
| Cdyn (mbar/mL) | 35 | 11 | 19 | 13 | ||||
| baseline | after lavage | RM | after injurious ventilation | RM | ||||
| II | PaO2 (mmHg) | 638 | 60 | 84 | 83.2 | 61.4 | 82.7 | -injurous ventilation was performed with tidal a volume of 17 ml/kg body weight for 3 hours -after injurious ventilation the animal deteriorated rapidly and could not be stabilized with e.g. bolus injections of epinephrine -the last blood gas analysis was obtained under ventilation with PEEP: 20 mbar. Ppeak: 35 mbar. resulting in a tidal volume of only 187 ml (4ml/kg body weight) – reduction of the injurious ventilation period was necessary in following experiments |
| PaCO2 (mmHg) | 41 | 78 | 77 | 85.1 | 120 | 183 | ||
| pH | 7.37 | 7.17 | 7.16 | 7.13 | 7.02 | 6.81 | ||
| Lactate (mg/dL) | 16 | 18 | 20 | 17 | 30 | 65 | ||
| heart rate (beats/min) | 86 | 64 | 109 | 133 | 150 | 185 | ||
| CO (L/min) | 4.3 | 3.3 | 3.7 | 5.6 | 2.4 | |||
| mAP (mmHg) | 77 | 82 | 61 | 53 | 77 | 40 | ||
| mPAP (mmHg) | 15 | 30 | 24 | 35 | 35 | 32 | ||
| PCWP (mmHg) | 7 | 8 | 9 | 8 | 9 | |||
| Cdyn (mbar/mL) | 34 | 9 | 12 | 17 | 14 | 13 | ||
Table 2: Arterial blood gases and hemodynamic data during implementation of the protocol. The table presents the respective arterial blood gases and hemodynamic data of two animals, which died prematurely during the implementation of the protocol. Gray background highlights the last results before death. RM: recruitment maneuver, PaO2: arterial partial pressure of oxygen, PaCO2: arterial partial pressure of carbon dioxide, CO: cardiac output, mAP: mean arterial pressure, mPAP: mean pulmonary arterial pressure, PCWP: pulmonary capillary wedge pressure, PEEP: positive end-expiratory pressure, Ppeak: peak inspiratory pressure.
