All vessels in the lower extremities can be visualized if this protocol is correctly performed (Figure 2A). In a hind-limb ischemia model, the non-ligated femoral artery runs parallel to the femoral vein (Figure 2B), and a ligated femoral artery can be confirmed by the interruption of contrast media (Figure 2C). The results revealed the development of collateral vessels (Figure 2D). Collateral circulation is formed between the arteries proximal to the ligated artery and the artery in the lower leg region and on the ventral and dorsal sides of the femoral artery. The inferior gluteal artery-beginning on the dorsal side of the pelvis and running on the lateral side of the thigh-expands robustly on the ischemic side.
Contrast-filled vessels are filled with the contrast medium (Figure 2E); disruption in the contrast indicates mixing of noncontrast media (e.g., blood, vasodilator buffer, or bubbles) or insufficient perfusion of the contrast (Figure 2F). Vasodilatation and fixation would not work well if the blood vessels have shrunk. Although CT imaging can only visualize the contrast medium, it is possible to view the arteries on the surface of the body by macroscopic or stereomicroscopic observation (Figure 2G). Thus, it is easier to assess defects using the contrast medium (Figure 2H).
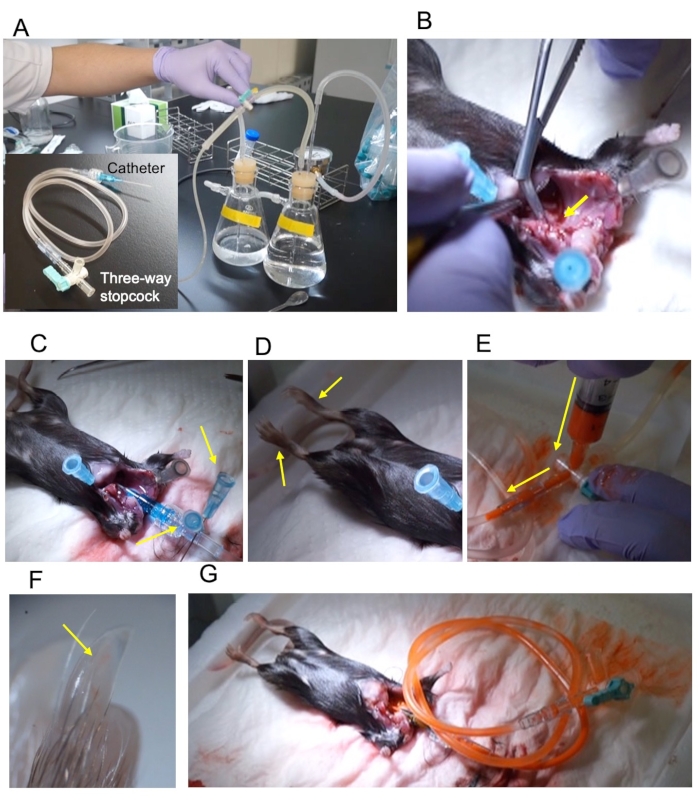
Figure 1: Outline of the procedure. (A) Pressure perfusion apparatus and the 22 G catheter connected via a 2 mL extension tube and three-way stopcock. (B) The ascending aorta is cut diagonally to expose the cross-section (yellow arrow). (C) The catheter was fixed using two pins (yellow arrows). (D) The fixed lower limbs extend upon fixation (yellow arrows). (E) Injection of contrast through the three-way stopcock. The injection direction is indicated by a yellow arrow. (F) The hind-limb nail is filled with the contrast (yellow arrow). (G) The stopcock is closed and removed from the perfusion apparatus. Please click here to view a larger version of this figure.
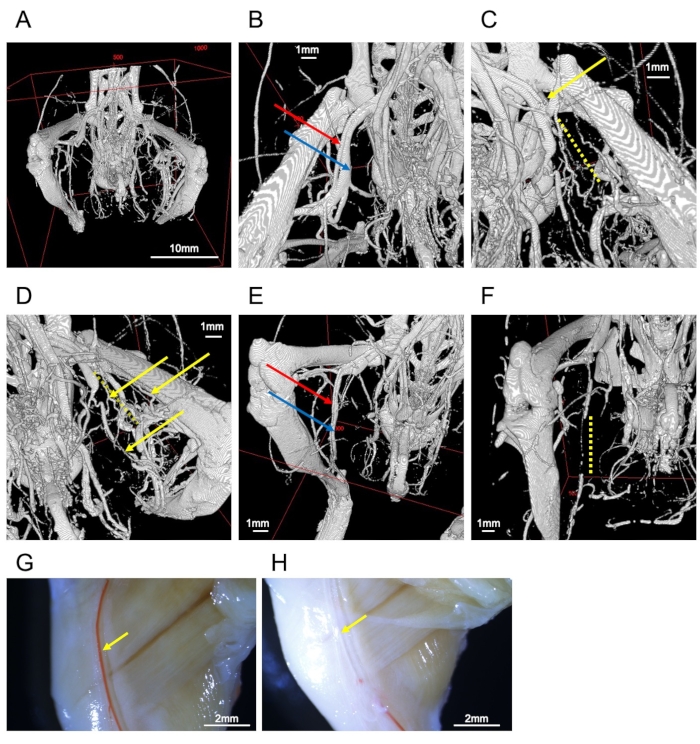
Figure 2: Images of vessels. (A) Whole image of the hind-limb bones and vessels. (B) Femoral artery (red arrow) and vein (blue arrow). (C) Ligated femoral artery (yellow arrow). The periphery is interrupted by the obstruction (yellow dotted line). (D) Collateral vessels in the ligated side (yellow arrows). The yellow dotted line represents the interrupted femoral artery. (E) A well-filled sample of the saphenous artery (red arrow) and vein (blue arrow). (F) Inadequate perfusion leads to interruption of saphenous vessels (yellow dotted line). (G) Stereomicroscopic observation of a representative sample. The right femoral artery (yellow arrow) is filled with contrast medium. (H) Stereomicroscope observation of a failed sample. The right femoral artery (yellow arrow) lacks contrast medium. Scale bars = 1 mm (B–F), 2 mm (G, H), 10 mm (A). Please click here to view a larger version of this figure.
