Endoscopic Ultrasound-Guided Biliary Drainage: Endoscopic Ultrasound-Guided Hepaticogastrostomy in Malignant Biliary Obstruction
Summary
Endoscopic Ultrasound-Guided Biliary Drainage (EUS-BD) is an alternative method of biliary decompression in malignant biliary obstruction. Here we describe the technique of EUS guided-Hepaticogastrostomy (EUS-HGS) in a case of unresectable malignant hilar biliary obstruction.
Abstract
Patients with unresectable malignant biliary obstruction often require biliary drainage to decompress the biliary system. Endoscopic Retrograde Cholangiopancreatography (ERCP) is the primary biliary drainage method whenever possible. Percutaneous Transhepatic Biliary Drainage (PTBD) is used as a salvage method if ERCP fails. Endoscopic Ultrasound-Guided Biliary Drainage (EUS-BD) provides a feasible alternative biliary drainage method where one of the methods is EUS guided Hepaticogastrostomy (EUS-HGS). Here we describe the EUS-HGS technique in a case of unresectable malignant hilar biliary obstruction to achieve biliary drainage.
Presented here is the case of a 71-year-old female with painless jaundice and weight loss for 2 weeks. Computed Tomography (CT) imaging showed a 4 x 5 cm hilar tumor with lymphadenopathy and liver metastasis. EUS fine needle biopsy (FNB) of the lesion was consistent with cholangiocarcinoma. Her bilirubin levels were 212 µmol/L (<15) during presentation.
A linear echoendoscope was used to locate the left dilated intrahepatic ducts (IHD) of the liver. The segment 3 dilated IHD was identified and punctured using a 19 G needle. Contrast was used to opacify the IHDs under fluoroscopic guidance. The IHD was cannulated using a 0.025-inch guidewire. This was followed by the dilation of the fistula tract using a 6 Fr electrocautery dilator along with a 4 mm biliary balloon dilator. A partially covered metallic stent of 10 cm in length was deployed under fluoroscopic guidance. The distal part opens in the IHD and the proximal part was deployed within the working channel of the echoendoscope that subsequently released into the stomach. The patient was discharged three days after the procedure. Follow up performed in the second and fourth weeks showed that the bilirubin levels were 30 µmol/L and 14 µmol/L, respectively. This indicates that EUS-HGS is a safe method for biliary drainage in unresectable malignant biliary obstruction.
Introduction
Patients with malignant biliary obstruction are often unresectable and advanced at presentation1,2. As a result, palliative endoscopic biliary decompression is often needed in managing these cases3,4,5. According to current recommendations, Endoscopic Retrograde Cholangiopancreatography (ERCP) is the primary method of biliary drainage, whenever possible, and if this fails or is contraindicated, Percutaneous Transhepatic Biliary Drainage (PTBD) is used as a salvage method6,7,8. However, there are certain complications associated with PTBD, which include septicemia, cholangitis, bleeding, electrolyte lost, leakage, wound infection, local discomfort; these complications are reported to be as high as 53.2%9. The emergence of Endoscopic Ultrasound-Guided Biliary Drainage (EUS-BD) provides a feasible alternative biliary drainage method to address this gap. The principal technique of EUS-BD involves the use of endosonographic imaging to guide access to the biliary system via the gastrointestinal tract to provide therapeutic decompression of an obstructed biliary system.
EUS-BD was first performed in 2001, and since then, this method of biliary drainage has evolved over the years10. Methods of EUS-BD commonly are EUS-guided choledochoduodenostomy (EUS-CDS), EUS-guided hepaticogastrostomy (EUS-HGS), EUS-guided Anterograde stenting (EUS-AS), and EUS-guided Rendezvous (EUS-RV)11,12. To date, the indications for EUS-BD include patients who have failed ERCP, patients having an inaccessible papilla by duodenal obstruction, and patients with altered surgical anatomy13,14,15.
EUS-HGS involves transmural drainage of the left intrahepatic duct into the stomach. The main advantage is that it provides internal drainage, which is more physiological and, most of all, offers better patients' comfort compared to PTBD12,16. This method is feasible for both hilar and distal malignant biliary obstruction. Here, we describe the technique of EUS-HGS as one of the methods of EUS-BD in a case of unresectable malignant hilar tumor.
A 71-year-old female was presented with painless jaundice and had a weight loss of 4 kg in 2 weeks duration. On examination, she was found to have scleral jaundice. Abdominal examination was unremarkable. Computed Tomography (CT) imaging showed a 4 x 5 cm hilar tumor involving the bifurcation of the right hepatic duct, the confluence of hepatic ducts and extrahepatic ducts, causing marked intrahepatic duct dilatation with lymphadenopathy and liver metastasis (Figure 1A). EUS fine needle biopsy (FNB) of the lesion was performed and it showed adenocarcinoma with positive CK7 and CA19-9 which was consistent with the diagnosis of hilar cholangiocarcinoma (Figure 1B). Her bilirubin levels were 212 µmol/L (<15) at presentation and CA19-9 levels were 305 U/mL. EUS-HGS was performed to provide relief in the biliary obstruction.
Protocol
The protocol was performed in accordance with the ethical guidelines of the University of Malaya Medical Center. Written consent was obtained, and a detailed explanation of the procedure was provided to the patient. Permission was also granted to produce the video of the procedure for educational purposes.
1. Positioning and sedation
- Place the patient in a prone position. Provide moderate sedation using intravenous infusion of Propofol. Ensure the infusion is titrated by the anesthetist.
2. Identifying the suitable target dilated left intrahepatic ducts
- Advance the linear echoendoscope making sure it passes the gastro-esophageal junction.
- Place the tip of the echoendoscope at the lesser curvature of the gastric cavity and proceed to identify the dilated left intrahepatic duct (IHD).
- Perform fluoroscopic imaging to ascertain the position of the echoendoscope. The tip of the echoendoscope must be placed at the lesser curvature of the gastric cavity, as stated previously. Always maintain the echoendoscope position and stabilize with periodic checks using fluoroscopic imaging throughout the procedure.
- Identify the dilated segment 3 IHD. Slightly tilt the angle of the tip of the echoendoscope upward to facilitate the next step in needle puncture.
NOTE: Subsequent steps of the procedure involve inserting and exchanging of accessories via the working channel of the echoendoscope throughout the procedure.
3. Needle access into the targeted dilated left intrahepatic duct
- Perform Doppler ultrasound to ensure that there are no intervening blood vessels around the targeted IHD.
- Using a 19 G needle, puncture the segment 3 IHD (Figure 2A). Using a 10 mL syringe preloaded with 7 mL of the contrast solution, gently aspirate the bile solution, this was to confirm the success of biliary access.
- Following that, perform contrast injection to opacify the left IHD and the rest of the biliary system.
4. Guidewire manipulation
- Use a 0.025-inch guidewire to navigate into the left IHD under the fluoroscopic guidance.
- Cannulate the guidewire across into the right intrahepatic duct (Figure 2B).
NOTE: Ideally, the guidewire should be manipulated deep into the common bile duct; however, it was not possible in this case due to the obstructing hilar tumor.
5. Fistula tract dilation
- Dilate the fistula tract using a 6 Fr electrocautery dilator in addition to using a 4 mm biliary balloon dilator (Figure 2C).
NOTE: Fistula tract dilation is required to facilitate insertion of the biliary stent later. - Perform balloon inflation for approximately 5 s.
NOTE: While doing these, monitor the position of the accessories monitored using both the sonographic and fluoroscopic image, ensuring that the wire is visible and the echoendoscope position is maintained. This is done to ensure a smooth transition during the exchange of accessories which is very important.
6. Stent insertion and deployment
- Deploy a 10 mm sized partially covered biliary stent (length of 10 cm) under fluoroscopic guidance (Figure 3A).
NOTE: The stent has a 3 cm uncovered distal portion and a 7 cm covered proximal portion. The uncovered part must be within the intrahepatic duct (Figure 3C). Approximately 3 cm of the covered part of the stent is left in the gastric cavity to prevent inward migration of the stent (Figure 3B). - Ensure that the distal end of the stent opens in the IHD. Deploy the proximal end within the working channel of the echoendoscope and subsequently release into the stomach with bile seen flowing within the stent.
Representative Results
The procedure was completed in approximately 30 min. There were no complications after the procedure and the patient was able to resume oral intake the next day. The bilirubin levels fell to 92 µmol/L and she was discharged three days after the procedure. A repeated CT imaging was done which showed the stent in position with a resolution of biliary obstruction. The bilirubin level on the follow-up was 30 µmol/L after 2 weeks post procedure and 14 µmol/L at 4 weeks post procedure (Table 1).
A total of 15 patients with unresectable malignant biliary obstruction underwent EUS-HGS in our institution between June 2020 to June 2021. The mean age was 65.5 (±10.1) years and 46.7% were males. Pancreatic cancer (46.7%) was the most common diagnosis and having altered surgical anatomy (33.3%) was the most common indication for the procedure. Clinical success was defined as a reduction of bilirubin levels of more than 50% within 4 weeks post procedure. The technical success rate, clinical success rate, and procedure-related adverse events were 86.7%, 81.8%, and 6.7%, respectively. The only case of procedure related adverse event was bleeding, which required transarterial embolization. One patient required re-intervention due to stent re-occlusion 102 days after the procedure in which a double pigtail plastic biliary stent was inserted via the existing metallic stent. Two patients died in less than 4 weeks due to advanced cancer. The results of our experience are shown in Table 2.
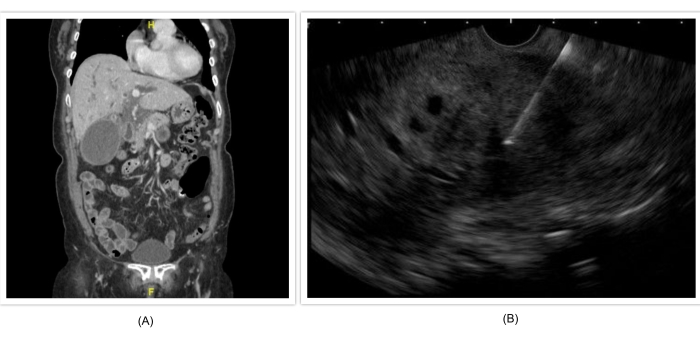
Figure 1: Showing the CT and EUS images of the hilar tumor. (A) CT scan showing dilated intrahepatic ducts. (B) EUS FNB of the tumor. Please click here to view a larger version of this figure.
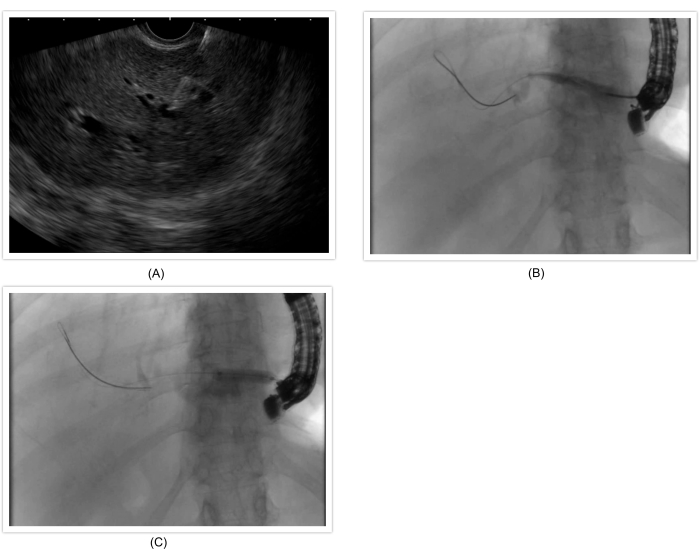
Figure 2: Illustrating the steps to access the left intrahepatic duct. (A) Needle access into the left intrahepatic duct. (B) Guidewire manipulation into the left intrahepatic duct. (C) Balloon dilation of the fistula tract. Please click here to view a larger version of this figure.
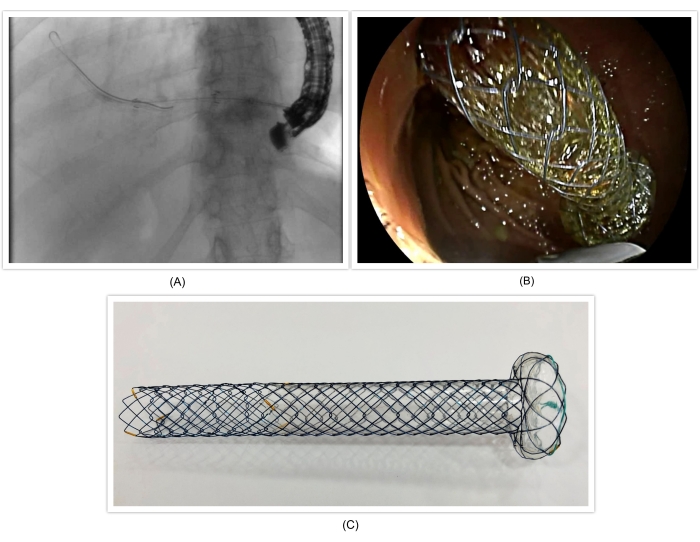
Figure 3: Showing the metallic stent and its deployment. (A) Stent deployment on fluroscopic view. (b) Stent deployment on endoscopic view (C) Partially covered metallic stent with a distal uncovered part and a proximal covered part with a flap. (Picture courtesy of MI Tech.) Please click here to view a larger version of this figure.
| Procedure Time | 30 mins |
| Days after the procedure (days) | Bilirubin Levels (µmol/L) |
| 0 | 212 |
| 3 | 92 |
| 14 | 30 |
| 30 | 14 |
Table 1: Results for the presented case.
| Variables | n = 15 |
| Mean Age, years (±SD) | 65.5 (±10.1) |
| Gender, n (%) | |
| Male | 7 (46.7) |
| Female | 8 (53.3) |
| Diagnosis, n (%) | |
| Pancreatic Cancer | 7 (46.7) |
| Cholangiocarcinoma | 3 (20.0) |
| Hepatocellular Carcinoma | 2 (13.3) |
| Gallbladder Cancer | 1 (0.7) |
| Metastatic Cancer | 2 (13.3) |
| Indication, n (%) | |
| Failed ERCP | 3 (20) |
| Inaccessible Papilla | 4 (26.7) |
| Altered Surgical Anatomy | 5 (33.3) |
| Primary Method | 2 (13.3) |
| Recurrent Biliary Obstruction post ERCP | 1 (6.7) |
| Level of Biliary Obstruction, n (%) | |
| Proximal | 4 (26.7) |
| Distal | 11 (73.3) |
| Technical Success Rate, n (%) | 13 (86.7) |
| Clinical Success Rate, n (%) | 9/11 (81.8) |
| Adverse Event, n (%) | 1 (6.7) |
| Re-intervention, n (%) | 1/13 (7.7) |
Table 2: Characteristics and results of patients who underwent EUS-HGS for unresectable malignant biliary obstruction.
Discussion
The above case description illustrates the possibility of using EUS-HGS as an alternative biliary drainage method in the management of biliary tract malignancies compared to existing methods such as ERCP and PTBD. Among the steps described above, identifying, and accessing the correct intrahepatic duct, guidewire manipulation, and stent deployment are the three main crucial steps in ensuring that the procedure can be performed successfully and safely.
In choosing the ideal liver segment for biliary access, both segment 2 and segment 3 IHDs can be targeted, but segment 3 is often preferred over segment 217. This is because in segment 2, there is a risk that the devices and accessories used will traverse through the esophagus and to the mediastinum leading to complications such as mediastinitis and pneumomediastinum18. In addition to that, the risk of the stent opening within the esophagus may lead to delayed esophageal perforation into the mediastinum19. Having said that, access via segment 2 is not contraindicated as long as the position of the echoendoscope is within the gastric cavity.
Guidewire manipulation within the intrahepatic ducts to its correct direction and position is arguably the most difficult and critical aspect of this procedure. The ideal position of the guidewire should be within the common bile duct or at least at the liver hilum to provide enough length and stability for the exchange of accessories without risking the guidewire slipping out from the insertion site17. In the above case, the guidewire was unable to pass through into the common bile duct due to proximal tumor obstruction but was able to go through into the right intrahepatic duct to provide an extra length of the wire and thus improve stability. A hydrophilic 0.035-inch guidewire or a 0.025-inch guidewire with a highly flexible tip that provides sufficient stiffness can be used17,20. Guidewire shearing within the fine needle aspiration (FNA) needle is not an uncommon problem and thus, extra caution should be taken when maneuvering it21. Options to dilate the fistula tract following successful wire cannulation include using an electrocautery device with or without a biliary bougie/balloon dilator, a 6 Fr electrocautery device is usually used, and fistula dilation should not exceed 8.5 Fr to avoid bile leakage. However, the frequency of bleeding is higher when using an electrocautery device dilator and hence some may prefer using only bougie/balloon dilators or a specific tapered tip biliary dilator22,23,24.
Regarding stent choices, fully covered self-expandable metal stents, partially covered metal stents, and plastic stents can be used for EUS-HGS25,26. Metal stents are often the preferred choice over plastic stents due to better stent patency and lower incidence of bile leak13. Dedicated partially covered hybrid metal stents such as the one used in this case have been increasingly used in this procedure. These stents consist of an uncovered intrahepatic distal portion and a covered gastric portion with a proximal anchoring flap to prevent inward stent migration and bile leak27,28,29. Intra-scope channel deployment of the stent is currently the preferred method of stent deployment to prevent stent migration as compared to extra-scope deployment30.
The technical success and clinical success rate of EUS-HGS on available studies, which are mostly retrospective, were 65% to 100% and 66% to 100%, respectively, whereas the rate of adverse events was 9.5% to 35.6%16,29,31,32,33,34,35,36,37,38. Bleeding is the most common adverse event, among others are peritonitis, cholangitis, pneumo-peritoneum, bile leak, and stent migration or stent re-occlusion14,16,36,39,40. These results were consistent with the experience in our institution. In comparison with existing biliary drainage methods, EUS-HGS is comparable to PTBD in terms of efficacy and safety but with fewer re-intervention and shorter hospital stay41. As a whole, EUS-BD is preferred over PTBD. This was reflected in a recent meta-analysis, which showed that EUS-BD has better clinical success, lower adverse events, and lower reintervention rates compared to PTBD42. Another advantage that EUS-BD has over PTBD is that it provides internal biliary drainage away from the tumor lesion and thus improves stent patency. Moreover, the majority of patients prefer EUS-BD over PTBD with the main reason being it provides internal drainage as opposed to an external one43. In the event of stent re-occlusion, reintervention via the existing stent placement can be done easily by either reinsertion of another metallic stent or a plastic biliary stent38. Therefore, if expertise is available, EUS-BD can be a salvage biliary drainage method when ERCP fails7,13,14. Having said that, this is promising evidence with regards to the use of EUS-HGS as a primary method of biliary drainage with good success38,44.
While EUS-HGS has shown to be a viable method of biliary drainage, there are limitations to its usage in routine clinical practice. Firstly, this is a complex procedure limited to centers with the expertise and those with a high case volume in advanced endoscopic ultrasound. Furthermore, there is a steep learning curve in training and performing this procedure45. With that in mind, it is recommended that this is done only by endoscopists with adequate training and experience in this procedure13,14. Patients' selection is also an important factor to consider when choosing this method of biliary drainage. EUS-HGS should not be performed in patients who are unfit for endoscopy, have a poor life expectancy or presence of coagulopathy, nor in the presence of ascites. In the presence of ascites, a mature fistula may not be established, which will result in peritonitis from bile and intestinal leaks14. Bleeding risk is often higher in EUS-BD as mentioned previously, though there are no clear recommendations with regards to the specific type of coagulopathy, EUS-BD should not be performed if the platelet levels are less than 50 x 109cells/L and/or an international normalized ratio (INR) of more than 1.546.
In conclusion, EUS-HGS is a feasible and safe method of biliary drainage in malignant biliary obstruction. At present, ERCP remains the primary method of biliary drainage and if it fails or is contraindicated, both EUS-HGS or PTBD can be considered. EUS-HGS may have some advantages over PTBD in that it provides internal drainage, fewer rates of adverse events and a lower rate of re-intervention. Having said that, all these methods should complement and coexist with each other to achieve good clinical outcomes. Further prospective studies are needed to compare these methods and their long-term outcomes.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors have no acknowledgments.
Materials
| 10mm in size, 10cm in length Partially Covered Metallic Stent | M.I Tech | BPD10100-E180 | |
| Curved Linear Echoendoscopy | Fujifilm | EG-580UT | |
| Electrocautary Dilator, 6Fr | G-Flex | CYSTO06U | |
| Endoscopic Ultrasound System Processor | Fujifilm | SU-1 | |
| Expect 19-guage FNA Needle | Boston Scientific | M00555500 | |
| Hurricane Biliary Balloon Dilator, 4mm | Boston Scientific | M00545900 | |
| Visiglide 0.025-inch Guidewire, 4500mm in length | Olympus | G-240-2545S |
References
- Rawla, P., Sunkara, T., Gaduputi, V. Epidemiology of pancreatic cancer: Global trends, etiology and risk factors. World Journal of Oncology. 10 (1), 10-27 (2019).
- Nagino, M., et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: A single-center 34-year review of 574 consecutive resections. Annals of Surgery. 258 (1), 129-140 (2013).
- Aadam, A. A., Liu, K. Endoscopic palliation of biliary obstruction. Journal of Surgical Oncology. 120 (1), 57-64 (2019).
- Boulay, B. R., Birg, A. Malignant biliary obstruction: From palliation to treatment. World Journal of Gastrointestinal Oncology. 8 (6), 498-508 (2016).
- Irisawa, A., Katanuma, A., Itoi, T. Otaru consensus on biliary stenting for unresectable distal malignant biliary obstruction. Digestive Endoscopy. 25, 52-57 (2013).
- Mukai, S., et al. Indications and techniques of biliary drainage for acute cholangitis in updated Tokyo Guidelines 2018. Journal of Hepato-Biliary-Pancreatic Sciences. 24 (10), 537-549 (2017).
- Dumonceau, J. M., et al. Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated 2017. Endoscopy. 50 (9), 910-930 (2018).
- Anderson, M. A., et al. The role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. Gastrointestinal Endoscopy. 77 (2), 167-174 (2013).
- Heedman, P. A., et al. Palliation of malignant biliary obstruction: Adverse events are common after percutaneous transhepatic biliary drainage. Scandinavian Journal of Surgery. 107 (1), 48-53 (2018).
- Giovannini, M., et al. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy. 33 (10), 898-900 (2001).
- Hara, K., et al. Endoscopic ultrasonography-guided biliary drainage: Who, when, which, and how. World Journal of Gastroenterology. 22 (3), 1297-1303 (2016).
- Khoo, S., Do, N., Kongkam, P. Efficacy and safety of EUS biliary drainage in malignant distal and hilar biliary obstruction: A comprehensive review of literature and algorithm. Endoscopic Ultrasound. 9 (6), 369-379 (2020).
- Teoh, A. Y. B., et al. Consensus guidelines on the optimal management in interventional EUS procedures: results from the Asian EUS group RAND/UCLA expert panel. Gut. 67 (7), 1209-1228 (2018).
- Isayama, H., et al. Clinical practice guidelines for safe performance of endoscopic ultrasound/ultrasonography-guided biliary drainage: 2018. Journal of Hepato-Biliary-Pancreatic Sciences. 26 (7), 249-269 (2019).
- Nakai, Y., et al. Endoscopic ultrasound-guided biliary drainage for unresectable hilar malignant biliary obstruction. Clinical Endoscopy. 52 (3), 220-225 (2019).
- Paik, W. H., Park, D. H. Outcomes and limitations: EUS-guided hepaticogastrostomy. Endoscopic Ultrasound. 8, 44-49 (2019).
- Ogura, T., Higuchi, K. Technical tips for endoscopic ultrasound-guided hepaticogastrostomy. World Journal of Gastroenterology. 22 (15), 3945-3951 (2016).
- Piraka, C., et al. EUS-guided transesophageal, transgastric, and transcolonic drainage of intra-abdominal fluid collections and abscesses. Gastrointestinal Endoscopy. 70 (4), 786-792 (2009).
- Kaneko, J., et al. Mediastinitis due to perforation by a metal stent after endoscopic ultrasound-guided hepaticogastrostomy: a rare complication. Endoscopy. 52 (06), 519-521 (2020).
- Kedia, P., Gaidhane, M., Kahaleh, M. Endoscopic guided biliary drainage: How can we achieve efficient biliary drainage. Clinical Endoscopy. 46 (5), 543-551 (2013).
- Ogura, T., et al. Liver impaction technique to prevent shearing of the guidewire during endoscopic ultrasound-guided hepaticogastrostomy. Endoscopy. 47, 583-584 (2015).
- Honjo, M., et al. Safety and efficacy of ultra-tapered mechanical dilator for EUS-guided hepaticogastrostomy and pancreatic duct drainage compared with electrocautery dilator (with video). Endoscopic Ultrasound. 7 (6), 376-382 (2018).
- Ogura, T., et al. Novel fine gauge electrocautery dilator for endoscopic ultrasound-guided biliary drainage: experimental and clinical evaluation study (with video). Endoscopy International Open. 7 (12), 1652-1657 (2019).
- Paik, W. H., et al. Simplified fistula dilation technique and modified stent deployment maneuver for EUS-guided hepaticogastrostomy. World Journal of Gastroenterology. 20 (17), 5051-5059 (2014).
- Dhir, V., et al. Endoscopic ultrasonography-guided biliary and pancreatic duct interventions. Digestive Endoscopy. 29 (4), 472-485 (2017).
- Umeda, J., et al. A newly designed plastic stent for EUS-guided hepaticogastrostomy: a prospective preliminary feasibility study (with videos). Gastrointestinal Endoscopy. 82 (2), 390-396 (2015).
- De Cassan, C., et al. Use of partially covered and uncovered metallic prosthesis for endoscopic ultrasound-guided hepaticogastrostomy: Results of a retrospective monocentric study. Endoscopic Ultrasound. 6 (5), 329-335 (2017).
- Leung Ki, E. -. L., Napoleon, B. EUS-specific stents: Available designs and probable lacunae. Endoscopic Ultrasound. 8, 17-27 (2019).
- Cho, D. H., et al. Long-term outcomes of a newly developed hybrid metal stent for EUS-guided biliary drainage (with videos). Gastrointestinal Endoscopy. 85 (5), 1067-1075 (2017).
- Miyano, A., et al. Clinical impact of the intra-scope channel stent release technique in preventing stent migration during EUS-guided hepaticogastrostomy. Journal of Gastrointestinal Surgery. 22 (7), 1312-1318 (2018).
- Dhir, V., et al. Multicenter study on endoscopic ultrasound-guided expandable biliary metal stent placement: Choice of access route, direction of stent insertion, and drainage route. Digestive Endoscopy. 26 (3), 430-435 (2014).
- Kawakubo, K., et al. Multicenter retrospective study of endoscopic ultrasound-guided biliary drainage for malignant biliary obstruction in Japan. Journal of Hepato-Biliary-Pancreatic Sciences. 21 (5), 328-334 (2014).
- Artifon, E. L. A., et al. Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: Is there any difference. Gastrointestinal Endoscopy. 81 (4), 950-959 (2015).
- Poincloux, L., et al. Endoscopic ultrasound-guided biliary drainage after failed ERCP: cumulative experience of 101 procedures at a single center. Endoscopy. 47 (9), 794-801 (2015).
- Khashab, M. A., et al. International multicenter comparative trial of transluminal EUS-guided biliary drainage via hepatogastrostomy vs. choledochoduodenostomy approaches. Endoscopy International Open. 4 (2), 175-181 (2016).
- Gupta, K., et al. Endoscopic ultrasound-assisted bile duct access and drainage: multicenter, long-term analysis of approach, outcomes, and complications of a technique in evolution. Journal of Clinical Gastroenterology. 48 (1), 80-87 (2014).
- Guo, J., et al. Endoscopic ultrasound-guided biliary drainage using a fully covered metallic stent after failed endoscopic retrograde cholangiopancreatography. Gastroenterology Research Practice. 2016, 9469472 (2016).
- Nakai, Y., et al. Long-term outcomes of a long, partially covered metal stent for EUS-guided hepaticogastrostomy in patients with malignant biliary obstruction (with video). Gastrointestinal Endoscopy. 92 (3), 623-631 (2020).
- Khan, M. A., et al. Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-Analysis. Digestive Diseases and Sciences. 61 (3), 684-703 (2016).
- Wang, K., et al. Assessment of efficacy and safety of EUS-guided biliary drainage: a systematic review. Gastrointestinal Endoscopy. 83 (6), 1218-1227 (2016).
- Sportes, A., et al. Endoscopic ultrasound-guided hepaticogastrostomy versus percutaneous transhepatic drainage for malignant biliary obstruction after failed endoscopic retrograde cholangiopancreatography: a retrospective expertise-based study from two centers. Therapeutic Advances in Gastroenterology. 10 (6), 483-493 (2017).
- Sharaiha, R. Z., et al. Efficacy and safety of EUS-guided biliary drainage in comparison with percutaneous biliary drainage when ERCP fails: a systematic review and meta-analysis. Gastrointestinal Endoscopy. 85 (5), 904-914 (2017).
- Nam, K., et al. Patient perception and preference of EUS-guided drainage over percutaneous drainage when endoscopic transpapillary biliary drainage fails: An international multicenter survey. Endoscopic Ultrasound. 7 (1), 48-55 (2018).
- Kongkam, P., et al. ERCP plus endoscopic ultrasound-guided biliary drainage versus percutaneous transhepatic biliary drainage for malignant hilar biliary obstruction: a multicenter observational open-label study. Endoscopy. 53 (01), 55-62 (2021).
- Oh, D., et al. Optimal biliary access point and learning curve for endoscopic ultrasound-guided hepaticogastrostomy with transmural stenting. Therapeutic Advances in Gastroenterology. 10 (1), 42-53 (2017).
- Ben-Menachem, T., et al. Adverse events of upper GI endoscopy. Gastrointestinal Endoscopy. 76 (4), 707-718 (2012).
