All patients had their biliary tract stones cleared successfully, with 58 patients (58/81, 72%) having bile duct stones completely removed after the first operation, 18 patients (18/81, 22%) requiring a second operation, and five patients (5/81, 6%) undergoing a third operation to completely remove the stones. Three patients had recurrent intrahepatic cholelithiasis in the 5th and 6th postoperative years. There were 56 patients (56/81, 68.7%) who underwent percutaneous liver surgery, as well as 25 patients (25/81, 31.3%) who underwent surgery by indwelling a sinus formed by a "T" tube.
The number of stones was equal to one in 70 patients (70/81, 86.6%), equal to two in eight patients (8/81, 10.4%), and greater than or equal to three in three patients (3/81, 3.0%). The stones were all cleared by using lithotomy forceps or a holmium-laser which is more effective in handling hard stones13. The patients required hospitalization at various times during their treatment course. Minor intraoperative biliary bleeding was observed in two patients, and one patient had a biliary infection after surgery, which extended the hospitalization cycle. The average hospital stay was 11 days (range 7-20 days). There was one complication of a small amount of reactive pleural effusion requiring admission (1/81, 1.2%), no deaths, and no massive hemorrhaging of the biliary tract (Table 2).
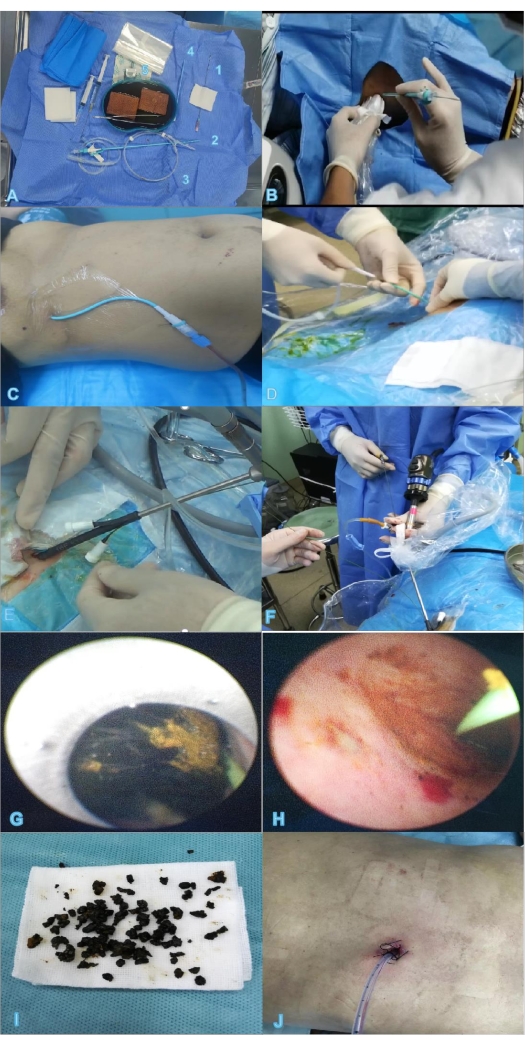
Figure 1: Two-step percutaneous transhepatic choledochoscopic lithotomy. (A) Instruments and materials required for PTCD, for example, puncture needle (1), trocar (2), guide wire (3), expander (4), blade (5). (B) Ultrasound-guided puncture. (C) Indwelling PTCD tube after successful puncture. (D) Insertion of the guide wire. (E,F) Insertion of the percutaneous nephroscope into the sheath to remove stones. (G) Removal of the stone under direct sight. (H) The stone is mostly removed. (I) The removed stone. (J) Two days after extubation, the wound has basically healed. Abbreviation: PTCD = percutaneous transhepatic catheter drainage. Please click here to view a larger version of this figure.
| Variables | n (%) N=81 |
| Age (years) | 66 (19-82) |
| Sex | |
| Male | 40 (49.4%) |
| Female | 41 (50.6%) |
| Surgical history | 60 (74.1%) |
| Principal complaint | |
| Stomachache | 9 (11.1%) |
| Stomachache + Jaundice | 14 (17.3%) |
| Stomachache + Fever | 22 (27.2) |
| Charcot triad | 36 (44.4%) |
| Child-Pugh score | |
| Grade A | 30 (37.0%) |
| Grade B | 51 (63.0%) |
| Grade C | 0 |
| Location of stone | |
| Left lobe | 3 (3.7%) |
| Right lobe | 4 (4.9%) |
| Bilateral | 6 (7.4%) |
| Common bile duct, CBD | 14 (17.3%) |
| CBD + Left lobe | 18 (22.2%) |
| CBD + Right lobe | 9 (11.1%) |
| CBD + Bilateral | 27 (33.4%) |
Table 1: Preoperative data. Abbreviation: CBD = common bile duct.
| Representative Results | Two-step PTCSL method | |
| N=81 | n% | |
| Stone extraction efficiency | 81 | 100% |
| Numbers of operations | ||
| 1 | 58 | 72% |
| 2 | 18 | 22% |
| 3 | 5 | 6% |
| Operation path | ||
| percutaneous transhepatic | 56 | 68.70% |
| "T" tube | 25 | 31.30% |
| Number of stones | ||
| 1 | 70 | 86.60% |
| 2 | 8 | 10.40% |
| ≥3 | 3 | 3.00% |
| Average hospital stay | 11 days | – |
| Complications | ||
| reactive pleural effusion | 1 | 1.20% |
| massive hemorrhage of the biliary tract | 0 | 0% |
| minor intraoperative biliary bleeding | 2 | 2.50% |
| biliary infection | 1 | 1.20% |
| fistula injury | 0 | 0% |
| drainage tube shedding | 0 | 0% |
| recurrence rate | 3 | 3.70% |
Table 2: Representative results. Abbreviation: PTCSL = percutaneous transhepatic choledochoscopic lithotomy.
| 0.9% Normal saline solution | – | ||
| 16-F series fascia dilator | type PLVW, Cook Medical | ||
| adjustable pressure pump | type APL; Guangzhou Jielun Medical Equipment Co. , Ltd, Guangdong Province, China | ||
| biliary balloon dilator | ATB advance; Cook Medical | ||
| blade | – | ||
| camera system | 1088i HD Camera Control Unit, PAL 220 V; Stryker Corporation | ||
| Cavity mirror protective sleeve | – | ||
| clamp | 5Fr, Richard Wolf GmbH, Germany | ||
| color ultrasound machine | DC-N2S, Mindray | ||
| Cook net basket | NGE-017115-MB, COOK Medical Inc. , Bloomington, USA | ||
| drainage pack | – | ||
| expander | – | ||
| guide wire | – | ||
| hydroelectric lithotripter | Aymed Medical,  stanbul, Turkey stanbul, Turkey |
||
| Iodophor | – | ||
| Kidney basin | – | ||
| light source | Voice-control compatible X8000 Xenon Light Source of 300 W;Stryker Corporation, MI | ||
| Medical syringe | – | ||
| puncture needle | – | ||
| suction apparatus | – | ||
| surgical gauze | – | ||
| trocar | – | ||
| Wolf nephroscope | 12-degree Ultra-Wide-Angle Ureteroreno-scope; Richard Wolf GmbH, Germany | ||
| zebra guide wire | type HAW; Cook Medical, Bloomington, IN |
