The contraction of the myocardial slices was displayed on the computer screen after insertion of the cultivation chamber into its corresponding connector (Figure 3). Contraction of the human myocardial slices started immediately upon stimulation. The slices hypercontracted for 5-10 min. This was visible as an increase of diastolic forces, caused by a tonic contracture of damaged tissue fractions. This process was reverted to varying degrees within 1-1.5 h. After stabilizing, human LV tissue slices showed twitch forces varying between 1 mN and 3 mN upon stimulation. Systole is shown as a strong increase in contraction force, followed by diastole with an equally steep decrease of the contraction force.
Contraction of the myocardial slices was recorded by the cultivation software and saved in a designated file. Each of the generated raw data files were converted to a readable Axon binary file format (.abf) for easy analysis and quantification of the data. For the initial analysis, the .abf file was opened in an appropriate program. Approximately 5 min of contraction data was selected to establish the average contraction amplitude during this period. This was done for multiple time points in the recorded data file. Plotting these contraction values over time yielded a useful graph to compare contraction development in a control and experimental setting. To gain a more advanced insight into the performance of the generated slices, stimulation protocols were run. During these protocols, which take approximately 45 min, the stimulation parameters were altered to assess parameters of contraction coupling.
The current stimulation protocol consisted of four distinct sections: post-pause-potentiation, stimulation threshold, force-frequency relation, and refractory period (Figure 4, Table 4). During the post-pause-potentiation, stimulation is resumed after a brief halt of either 3, 12, 50, or 120 s. To determine the stimulation threshold, the stimulation current is increased in steps of 3 mA every 10 s, starting at 8 mA and increasing to 90 mA. With this test, the minimal stimulation current can be determined for each slice. This does not alter the general stimulation settings outside of the stimulation protocol. The force-frequency relation is assessed by a stepwise increase of the stimulation frequency (20, 30, 45, 60, 80, 100, 120, 150, 180, 210, and 240 BPM), while the respective duration of each step is shortened in parallel. Except for the first two frequency settings, this regimen yields between 20-40 contractions during each step. The refractory period of each slice is assessed by sending a premature stimulus (S2) after a normal stimulus (S1; 30 BPM). The S1-S2 interval is shortened every 10 s.
To demonstrate the potential of the presented cultivation system as a tool for testing pharmacological interventions, ex vivo human LV tissue slices were prepared from the same patient and subjected to pharmacological agents that influence the intracellular calcium ion (Ca2+) levels (n = 1) after 2 weeks of cultivation. The L-type Ca2+-channel antagonist nifedipine inhibits Ca2+ influx into the myocardial cells and therefore lowers the intracellular availability of Ca2+ and reduces the contractility17. Because of its vasodilator action, nifedipine is used as an anti-hypertensive drug. To demonstrate pharmacological differences of Ca2+-channel antagonists, calciseptine was investigated for comparison. Calciseptine is also an L-type Ca2+-channel antagonist, extracted from the Dendroaspis p. polylepis venom18. Therefore, it shares the negative inotropic action of nifedipine. However, calciseptine has different binding characteristics and is more potent compared to nifedipine19. In order to study the positive and negative modulations of Ca2+ availability, we also tested the calcium channel agonist Bay-K8644 (1,4-Dihydro-2,6-dimethyl-5-nitro-4-(2-[trifluoromethyl]phenyl)pyridine-3-carboxylic acid methyl ester)20.
Three slices were treated with nifedipine (125 nM), calciseptine (70.8 nM), and Bay-K8644 (417 nM) respectively, while the fourth slice received no drug (control). The contraction forces under general stimulation parameters (50 mA current, biphasic pulses 3 ms duration, 1 ms interval, and 30 BPM pacing rate) were compared before and after treatment. Furthermore, before the treatment, a stimulation protocol was run to assess the baseline values for post-pause-potentiation, stimulation threshold, force-frequency relation, and refractory period. After 30 min of treatment, a second stimulation protocol was run. To eliminate inter-individual differences, contraction amplitude of each slice was normalized to its baseline level before treatment. The baseline (i.e., 100%) was determined by analyzing the last five contraction cycles before the start of the pre-treatment stimulation protocol.
When analyzing the contraction of the slices at general stimulation, it was observed that the contraction force of the slices treated with Ca2+ antagonists (nifedipine and calciseptine) decreased within 10 min post-treatment (Figure 5) and the effect was present up to 20 min post-treatment. In contrast, the voltage gated Ca2+ channel agonist Bay-K8644 increased the contraction force of the treated slice. The control slice did not show a noteworthy change. The contraction data generated during the stimulation protocols were analyzed in a similar way. Here, the data generated by the stimulation protocol performed before the treatment (pre-treatment) was compared to the post-treatment data of the same stimulation protocol.
As discussed before, the stimulation protocol started with the assessment of the post-pause-potentiation. During the pause, additional Ca2+ is taken up by the sarcoplasmic reticulum (SR), which is released upon first stimulation after the pause. Hence, post-pause-potentiation reflects intracellular Ca2+ release from the SR. As such, this parameter can be used to assess the relative contribution of Ca2+ released from the SR by the ryanodine receptor. To assess the potentiation of the slices after a stimulation pause, the strength of the first contraction after the pause was divided by the average contraction before the respective pause. The control slice did not show any noteworthy change (Figure 6A). It was observed that the inhibition of the L-type Ca2+ channels led to potentiation of the first contraction after a pause of at least 50 s (Figure 6B,D), reflecting a higher relative contribution of intracellular Ca2+ release to total contractility. The opposite effect was seen in the slice treated with Bay-K8644, which stimulates the entry of extracellular Ca2+ via the L-type Ca2+ channels (Figure 6C).
The force-frequency relation was assessed by successively increasing the pacing rate up to 180 BPM. For better visualization, the contraction force at different stimulation frequencies was normalized to the baseline contraction at 30 BPM within the same protocol (=100%). Data analysis showed that the treatment with calciseptine did not change the ability of the slice to follow the stimuli upon increase of the stimulation frequency when comparing the pre- and post-treatment data (Figure 7B). No change was observed in the control slice (Figure 7A). Contrary to calciseptine, nifedipine prevented an increase of contractility at higher pacing rates and reduced the maximum capture rate to 80 BPM (Figure 7D). The slice treated with the Ca2+ channel agonist Bay-K8644 showed an increased contraction force at very low stimulation frequencies (Figure 7C). However, at frequencies higher than 50 BPM, the contraction force appeared to be lower than during the pre-treatment condition. The stimulation threshold and the refractory period were also determined pre- and post-treatment. However, no differences were observed, and the data are therefore not shown.
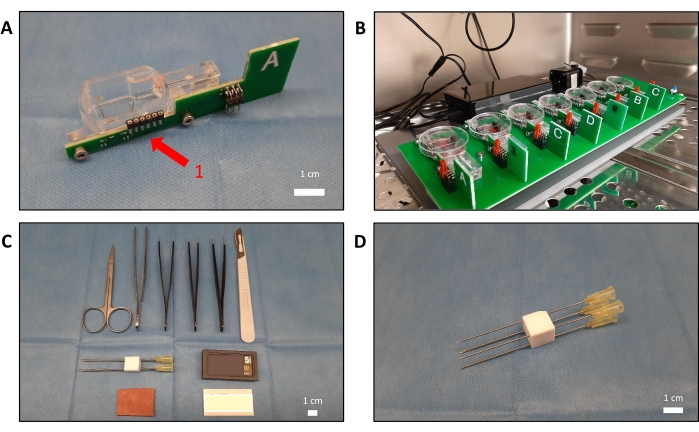
Figure 1: Overview of the required materials and the cultivation system. (A) An empty cultivation chamber connected to a green circuit board. The circuit board (1) measures the contraction with a sensor and transmits the data to the controller. (B) Eight filled chambers placed on the rocking main plate. Petri dish lids (35 mm) are used to cover the chambers. (C) The (surgical) tools needed to trim the transmural myocardial sample. Depicted are various tweezers, the blades needed for the vibratome, and a rubber patch to aid in trimming. (D) Four 0.9 mm x 70 mm 20 G needles that are fixed in a square position (0.9 cm x 0.9 cm) by a solid block of plastic. Using this construct prevents damage and movement of the sample when trimming and yields a tissue block with the required dimensions. Please click here to view a larger version of this figure.
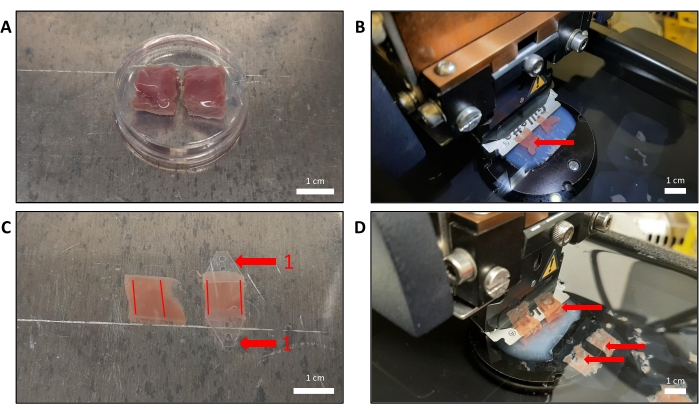
Figure 2: Processing of two LV samples. (A) Two myocardial tissue blocks (approximately 1 cm x 1 cm x 1 cm) embedded in solidified low-melt agarose in a 35 mm Petri dish. For demonstration purposes, porcine LV tissue was used. (B) The agarose block with the embedded samples was removed from the Petri dish, trimmed, and glued onto the cutting platform of the vibratome. Here, porcine LV tissue was used for demonstration purposes. Notice the uniform tissue color and the absence of white fibrotic tissue, indicated by the red arrow. (C) After slicing, the agarose is carefully removed, and plastic triangles (1) are connected perpendicular to the direction of the myocardial fibers. The red lines indicate the direction of the myocardial fibers. (D) Human LV tissue was prepared, which showed white fibrotic tissue within the slices. This does not necessarily lower the success rate of cultivation; however it is recommended to use slices that do not display fibrosis. Please click here to view a larger version of this figure.
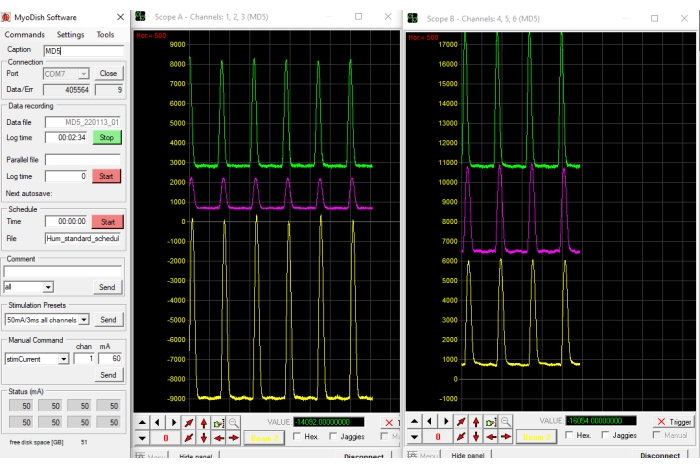
Figure 3: The cultivation software. Depending on the number of channels used (maximum of eight), the contraction registration will be visualized in up to three designated windows (two visible in the figure). Each cultivation chamber is displayed as one contraction graph. In the settings window, stimulation parameters can be altered and tailored to the desired experimental situation. This window also allows to start or stop the stimulation protocol/schedule that is selected. Please click here to view a larger version of this figure.
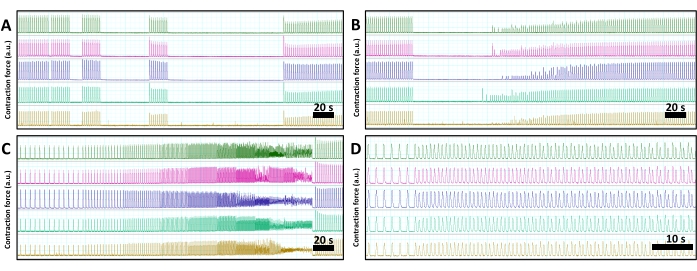
Figure 4: Read-out of the contraction of five myocardial slices during a typical stimulation protocol. In all panels, each individual slice is shown in the same color. (A) Post-pause-potentiation assesses the first contraction after a brief stimulation pause of 3, 12, 50, and 120 seconds respectively. (B) Determination of the stimulation threshold by increasing the stimulation current in steps of 3 mA every 10 s from 8 mA to 80 mA. (C) The force-frequency relation of each slice is assessed by stepwise increases of the stimulation frequency from 12 BPM to 240 BPM. The duration of stimulation periods becomes shorter at higher frequencies to keep the number of beats constant at each frequency. (D) To assess the refractory period, the slices are exposed to premature stimulations (S2) at decreasing intervals to the preceding stimulus (S1). Please click here to view a larger version of this figure.
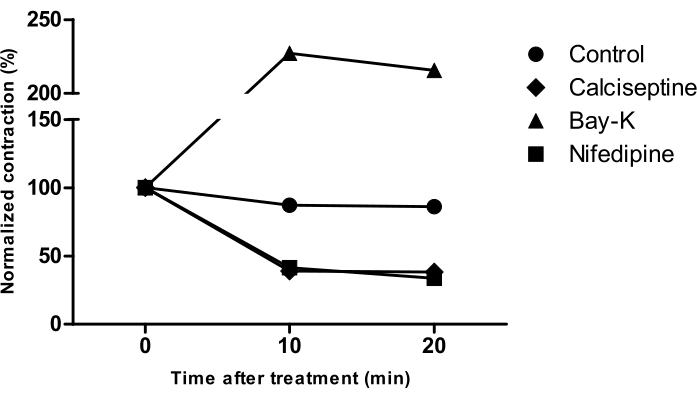
Figure 5: Analysis of contraction force before and after treatment with L-type Ca2+ channel affecting agents. All data (n = 1) were normalized to the baseline contractility (mean of five separate beats before treatment (0)). L-type Ca2+ channel antagonists nifedipine (125 nM), calciseptine (70.8 nM), and L-type Ca2+ channel agonist Bay-K8644 (417 nM) were added to contracting human LV myocardial slices. The control slice received no treatment. Please click here to view a larger version of this figure.
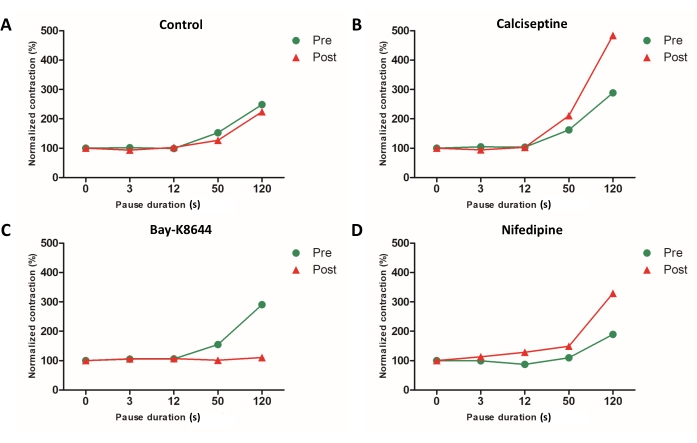
Figure 6: Post-pause-potentiation of the treated and control slices. Differences in post-pause-potentiation were observed (baseline vs post-treatment; n = 1). Here, the amplitude of the first contraction after a pause was normalized to the average contraction amplitude before the respective pause. Baseline was set as 100% and resembles the average contraction strength of the last five cycles before the first pause commences. The Y-axis displays the normalized first contraction after a pause of various durations. The X-axis shows the baseline and pause lengths. (A) Control slice without treatment. (B) Calciseptine treatment. (C) Bay-K8644 treatment. (D) Nifedipine treatment. Please click here to view a larger version of this figure.
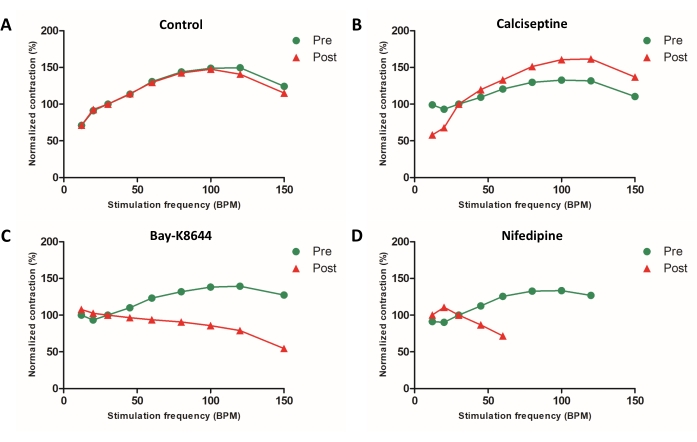
Figure 7: Analysis of the force frequency relation. Contraction data (n = 1) was normalized to the contraction force at 30 BPM within the respective protocol (= 100%). (A) The control slice was not treated with any substance; however, all other aspects of the cultivation were the same as those of the treated slices. (B) Calciseptine treatment of one LV myocardial slice. (C) Bay-K8644 treatment. (D) Nifedipine treatment. Data about the contraction force of this slice during stimulation frequencies above 80 BPM were omitted, as the contraction was not following the stimulation frequency. Please click here to view a larger version of this figure.
Table 1: Composition of the slicing buffer used for transport and during the slicing procedure. For the preparation of agarose, glucose is omitted. Please click here to download this Table.
Table 2: Composition of the 4% agarose gel. This glucose-free low-melt agarose gel is used for embedding of the tissue samples. Please click here to download this Table.
Table 3: Preparation of the medium for cultivation. Please click here to download this Table.
Table 4: Details of the stimulation protocol. The stimulation protocol consists of four parts, which all can be altered to suit the needs of the project. Please click here to download this Table.
