Patient characteristics
In this analysis, a total of 164 patients were identified who underwent radiofrequency PVI between January 2020 and January 2022. Patients were included regardless of whether they received only PVI or received additional lesions such as roof lines, floor lines, mitral isthmus lines, etc. LET monitoring was performed with a single-sensor temperature probe and was performed by the same teams and in the same labs as the cases with active cooling. There were 63 patients who received LET monitoring for their PVI during the study period and 101 patients who received active esophageal cooling for esophageal protection. There were similar proportions of AF type in both groups (Table 1).
Procedure duration and procedure variability
Procedure duration was defined as the time from the first sheath placed to the time of the last sheath removal. The mean procedure time in patients that underwent LET monitoring was 176 min ± 52 min. In the actively cooled group, the mean procedure time was 156 min ± 40 min, representing a 20 min overall reduction in procedure duration (P = 0.012). The median procedure time was 172 min (interquartile range [IQR] = 144 to 198 ) in the LET monitored group, and 151 min (IQR = 129 to 178 ; P = 0.025) in active esophageal cooling group. Overall, there was a median reduction of 21 min (FIGURE 1). Other than differences in the operator, no other factors differed between the groups other than the type of esophageal protection utilized. As such, the difference in procedural duration is believed to be due entirely to the pauses required with LET monitoring, reacting to temperature elevations, as well as the need to reposition repeatedly while ablating around the pulmonary veins. Although a long-term efficacy analysis has not yet been performed at this clinical site, data from elsewhere have shown improved efficacy with cooling when compared to LET monitoring. This is believed to be due to the improved point-to-point lesion sequencing that can be completed without interruption from local overheating alarms.
In the context of the technique described here, these results highlight the utility of the technique of workflow analysis, human factors analysis, and contextual inquiry to facilitate uncovering and analyzing data that can provide important insights into clinical practice. Traditional analyses of this type often rely on the manual extraction of large quantities of data, adding time and cost burdens to clinical investigations while reducing reliability and consistency. Incorporating advanced informatics techniques as described here opens new avenues for investigation without requiring extensive time and funding.
| Esophageal Protection | |||
| Active Esophageal Cooling (n=101) | LET Monitoring (n=63) | ||
| Patient age (years), mean (SD) | 67.9 ± 11.3 | 64.5 ± 11.6 | |
| Gender | Male | 66 | 46 |
| Female | 35 | 17 | |
| AF Type | Paroxysmal Atrial Fibrillation | 55 | 36 |
| Persistent Atrial Fibrillation | 38 | 23 | |
| Long-standing Persistent Atrial Fibrillation | 8 | 4 | |
Table 1: Patient characteristics, including age, gender, and type of atrial fibrillation treated.
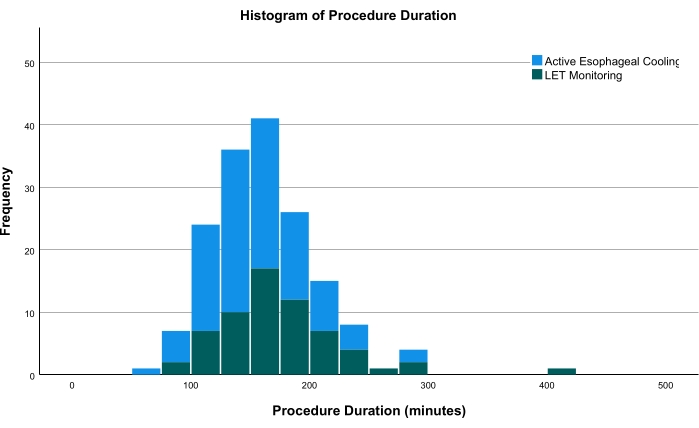
Figure 1: Histogram comparing the procedure times of both groups. The green bars show patients receiving LET monitoring; the blue bars show patients receiving active esophageal cooling. Abbreviation: LET = luminal esophageal temperature. Please click here to view a larger version of this figure.
Supplementary File 1: REDCap data storage extraction form. An example of the data extraction form used for this protocol, demonstrating the specific data elements recorded. Please click here to download this File.
