The procedure was performed in a conventional OR, equipped with a radiolucent OR table, a navigation platform, and a mobile CBCT device providing both 2D fluoroscopy and 3D CBCT images of high quality for AR navigation. Two porcine cadavers, which were approximately 80 cm in length and 45 kg, were used for the purpose of this study. The specimens were purchased commercially, and their use for this experiment did not require an ethical permit. All the devices, instruments, and software used within the described workflow are listed in the Table of Materials. The following step-by-step procedure was performed and repeated for each specimen.
1. Porcine cadaver specimen
- Place the porcine cadaver specimen on the operating table in the operating room.
- Drape the porcine cadaver specimen in sterile covers. Use incision film to cover the skin in the surgical field.
2. Identification of the vertebral levels of interest
- Using the CBCT scanner, identify the vertebral levels of interest by fluoroscopy. Use the wireless control tablet of the CBCT scanner to move the scanner to the desired position, align the x-ray beam, and to perform the fluoroscopy scan (Figure 1).
NOTE: The 2D scans can be immediately reviewed on the tablet. The vertebral levels are identified by looking for ribs on the fluoroscopy scan and counting upward or downward. - Attach the radiolucent navigation dynamic reference clamp to a spinous process in the area of interest by exposing the spinous process and fastening the clamp using the dedicated screwdriver. Then, attach the reflective spheres of the reference frame to the clamp (Figure 2).
- Perform a CBCT scan, and transfer the scan to the navigation platform (via LAN) (Figure 3). The navigation system camera tracks the CBCT scanner and the dynamic reference frame, enabling automatic patient registration using the Brainlab Loop-X Automatic Registration software on the navigation platform.
- Start the Spine & Trauma Navigation software on the navigation platform. Use the spinal pointer and the 2D navigation views to verify the accuracy of the patient registration on anatomical landmarks.

Figure 1: The wireless control tablet of the CBCT scanner. The tablet showing the fluoroscopy images from the CBCT. Please click here to view a larger version of this figure.

Figure 2: A schematic picture of the clamp attached to the spinous process. Please click here to view a larger version of this figure.

Figure 3: The Loop-X CBCT. The CBCT performing a scan on the draped pig cadaver with the reference attached. Please click here to view a larger version of this figure.
3. Instrument calibration
- Calibrate a navigated drill guide and a screw driver to the navigation system. For this purpose, select the instrument in the Brainlab Spine & Trauma Instrument Setup software, and then present the real instrument to the camera of the navigation system along with a calibration device. Move the instrument in a rotating motion while in contact with the calibration device until the navigation system recognizes the instrument. Once calibrated, track and visualize the instrument on both the 2D images and the 3D model in the HMD.
4. Head-mounted device fitting
- Ensure that each surgeon is fitted with a Magic Leap headset (the HMD). Ensure the HMD and the navigation platform are connected to the same network (WLAN connection for the HMD and LAN connection for the navigation platform).
- To establish the communication between the HMD and the Spine & Trauma Navigation software, look at the QR code displayed on the screen of the navigation platform. This starts the corresponding Mixed Reality application running on the HMD and transfer of data to the HMD.
- Perform the mixed reality alignment by looking at the spine reference array through the HMD for a few seconds. Wait for a 3D model of the spine, rendered based on the CBCT scan, to be accurately augmented onto the specimen in the HMD. In addition to the 3D overlay, look at the 2D navigation views and a second 3D model above the 2D navigation views (hover view) that are displayed in the HMD.
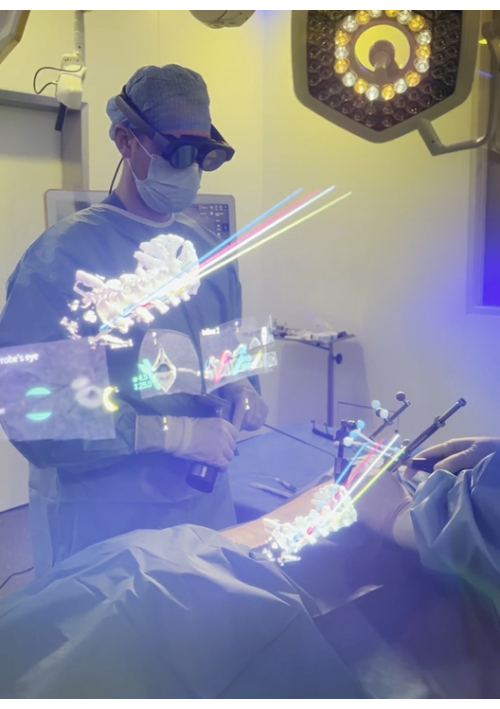
Figure 4: The view through the HMD. The surgeon's view through the HMD presenting both 2D and 3D information. The 3D overlay shows the planned 3D screws with protruding trajectory lines assisting instrument alignment. The lower 3D model is augmented onto the spine of the pig; additional information is provided in the 2D and 3D representations floating above, which can be positioned freely in the virtual space and switched on and off. Please click here to view a larger version of this figure.
5. Planning the pedicle screw placement
- Plan the pedicle screw paths based on the 3D registered augmented model, aligning them with the anatomy of the spine, and visualize in the HMD (Figure 5). Perform fine-tuning of the screw paths on the touchscreen of the navigation platform.

Figure 5: Pedicle screw path planning. The paths for the pedicle screws being planned using the HMD and the navigation pointer. Please click here to view a larger version of this figure.
6. Beginning the pedicle screw placement
- Make small skin incisions approximately 2 cm long with a scalpel for minimally invasive access to the pedicles based on the superimposed 3D model visible through the HMD (Figure 6).
- Using a minimally invasive technique, dissect the soft tissue, and dilate the canal with dilators until the pedicle entry point on the vertebral surface is reached.
- Adjust the depth of the drill guide to match the length of the screw planned for the pedicle. The planned screw length is displayed on the screen of the navigation system. Position and align the navigated drill guide to the planned path.
- Drill the pedicle using a power drill with a 4.5 mm drill bit (Figure 7). Drill according to the planned path; the drill guide stops the drill from going deeper than the planned depth.
- Estimate the time from the skin incision until the canal is drilled for each pedicle.
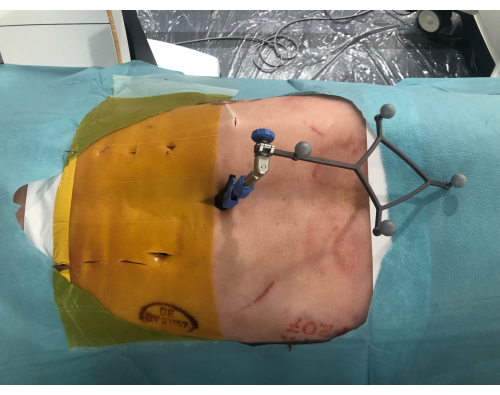
Figure 6: Minimally invasive incisions. The pig cadaver from above showing the minimally invasive incisions along the spine. To the right is the reference with the reflective spheres clamped to the spinous process. Please click here to view a larger version of this figure.

Figure 7: Drilling the pedicles. The pedicle is drilled with a power drill using the navigation visible through the HMD to align the drill guide to the pre-planned path. Please click here to view a larger version of this figure.
7. Visualization of the screw placement
NOTE: No screws were placed to avoid metal artifacts during evaluation.
- Perform a second CBCT to acquire X-ray images of the drilled vertebrae for the accuracy analysis. Ensure the drilled canal in the vertebra is clearly visible before using it for subsequent accuracy analyses.
8. Cannulating the spine
- Repeat the above procedure described in section 2, section 4, section 6, and section 7 to cover the next region of interest until the whole spine is cannulated.
- Repeat the same procedure (sections 1-8) using the second specimen.
9. Image analysis
- Match the obtained CBCT images to the navigation plan and make corrections according to the laboratory notes taken during the procedure.
- Have an independent reviewer evaluate all the images and grade the cannulations according to the Gertzbein grading scale, from 0 to 3. Grades 0 or 1 are considered accurate. Grades 2 or 3 are considered inaccurate.
- Fuse the trajectories of the planned paths and the cannulations, and define the technical accuracy as the deviation from the path at the entry and target. Measure the angular deviation.
In total, 33 navigated cannulations were performed. The time per cannulation and the clinical and technical accuracy were assessed on the postoperative CBCT scans (Figure 8).
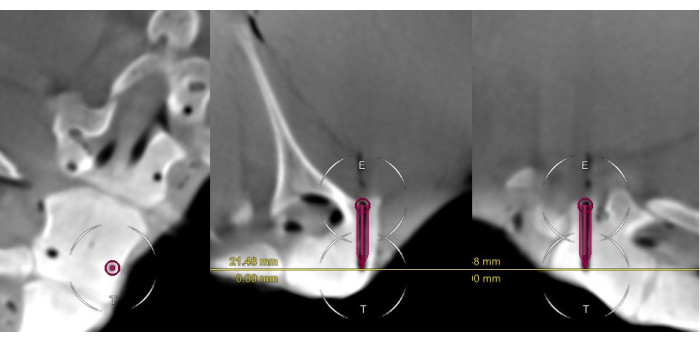
Figure 8: The postoperative scan of a Gertzbein grade 0 cannulation. The scan includes the surgical plan for the pedicle cannulation, presented in the coronal, axial, and sagittal views. Note the close alignment of the virtual screw and the cannulated canal. Please click here to view a larger version of this figure.
The mean insertion time per cannulation was 141 s ± 71 s (median [range]: 151 [43-471]; Figure 9).
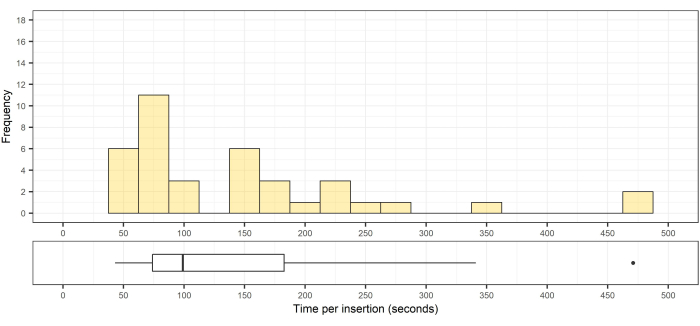
Figure 9: Histogram and box of the distribution of the pedicle cannulation times. Top, histogram of the distribution of the pedicle cannulation times (n = 33); bottom, the corresponding box plot showing the median, interquartile range, and an outlier. Please click here to view a larger version of this figure.
All 33 cannulations were considered clinically accurate according to the Gertzbein grading scale (32 grade 0; 1 grade 1; Table 1).
| Gertzbein Grade 0 | Gertzbein Grade 1 | Gertzbein Grade 2 | Gertzbein Grade 3 | Clinically Accurate | Clinically Inaccurate | Accuracy | |
| Number of screws | 32 | 1 | 0 | 0 | 33 | 0 | 100% |
Table 1: Clinical accuracy of implanted screws according to the Gertzbein grading scale. Grades 0 or 1 were considered accurate. Grades 2 or 3 were considered inaccurate.
To assess the technical accuracy, the deviation of each cannulation from its planned path was measured at the bone entry and at the bottom of the drill canal (Figure 10). The 3D measurements were performed by fusing the intraoperative scan, including the planned cannulation paths, with the postoperative scan of the cannulations. The angular deviation was calculated based on these data.
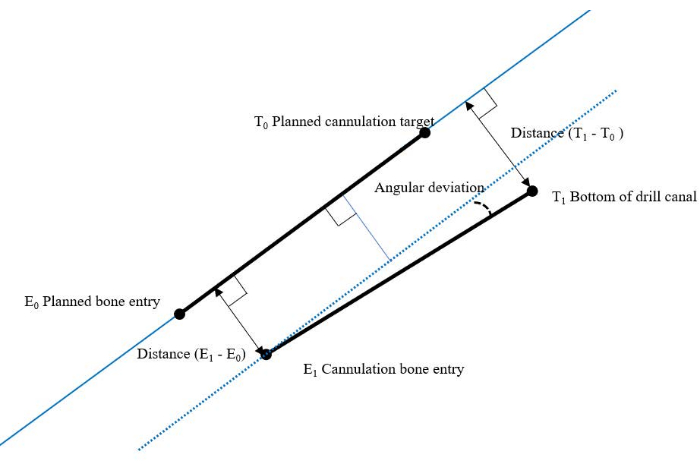
Figure 10: Overview of the measurement model for technical accuracy. Please click here to view a larger version of this figure.
This method was previously described by Frisk et al.12. For the 33 pedicle cannulations performed, the technical accuracy was 1.0 mm ± 0.5 mm (median [range]: 1.0 [0.4-3.3]) at the entry point (Figure 11) and 0.8 mm ± 0.1 mm (median [range]: 0.8 [0.6-4.6]) at the bottom of the drill canal (Figure 12). The angular deviation was 1.5° ± 0.6° (median [range]: 1.5 [0.3-5.0]; Figure 13).
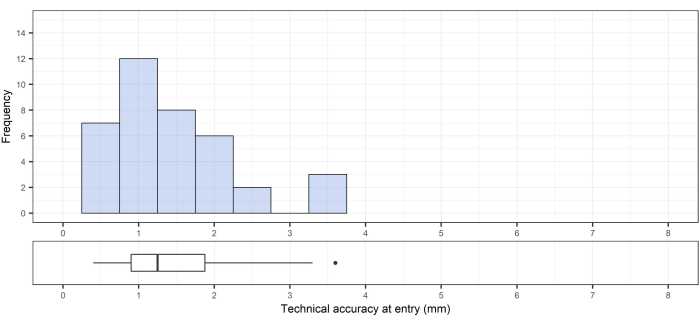
Figure 11: Technical accuracy at the bone entry point. Top, the technical accuracy at the entry; bottom, the corresponding box plot showing the median, interquartile range, and an outlier. Please click here to view a larger version of this figure.
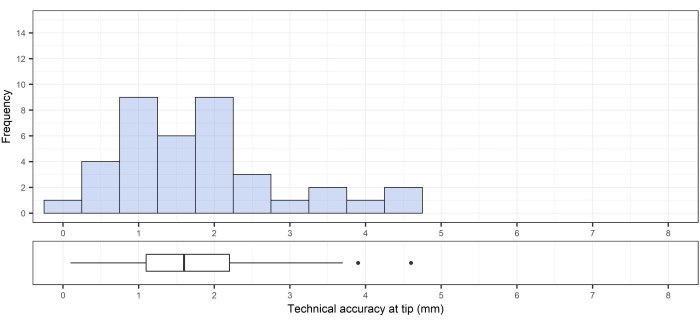
Figure 12: Technical accuracy at the target (tip of drill canal). Top, technical accuracy at the target (tip of the drill canal); bottom, the corresponding box plot showing the median, interquartile range, and outliers. Please click here to view a larger version of this figure.
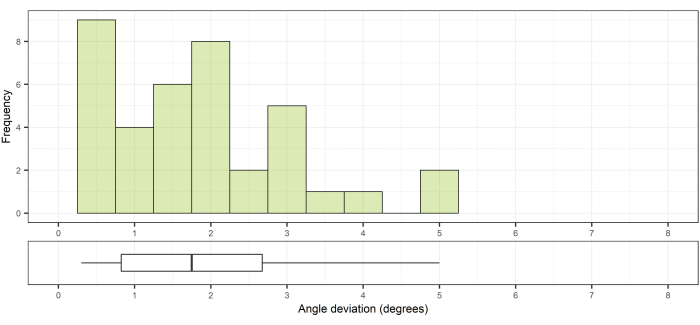
Figure 13: Angular deviation compared to the planned path. Top, angle deviation from the planned path; bottom, the corresponding box plot showing the median and interquartile range. Please click here to view a larger version of this figure.
| Instrument tracking array spine & trauma 4-marker | Brainlab | ||
| Curve Navigation System | Brainlab | Navigation System |
|
| Disposable clip-on remote control | Brainlab | SmartClip | |
| Drill guide tube, handle with marker spheres, drill guide depth control insertable, drill bits | Brainlab | Drill guide and accessories | |
| Expedium | DePuy Synthes | Screwdriver |
|
| Instrument calibration matrix | Brainlab | Instrument Calibration Matrix |
|
| Loop-X | Brainlab | CBCT scanner |
|
| Magic Leap 2 | Magic leap Inc. | Mixed Reality headset |
|
| Navigation pointer spine | Brainlab | Navigation Pointer |
|
| Spine reference array for reference clamp carbon (4-Sphere Geometry) | Brainlab | Spine Reference Array |
|
| Spine reference clamp carbon with slider | Brainlab | Spine Reference Clamp  |
|
| TruSystem 7500 | Trumpf | Operating table | |
| Software | |||
| Mixed Reality Spine Navigation App for Magic Leap | Brainlab | Run on Curve Navigation System Version: 2.0 |
|
| PDM | Brainlab | Run on Curve Navigation System Version: 4.2 |
|
| Spine & Trauma Instrument Setup | Brainlab | Run on Curve Navigation System Version: 6.2 |
|
| Spine & Trauma Navigation 2.0 | Brainlab | Run on Curve Navigation System Version: 1.6 |
