This study was carried out in strict accordance with the national standards for human experimentation, and the clinical study was approved by the Ethics Association of Xiangya Boai Rehabilitation Hospital (ethics approval number: 20211223). The children's guardians agreed to participate in this training program and signed informed consent forms. Children with SCP were recruited in the Xiangya Boai Rehabilitation Hospital and Xiangya Hospital of Central South University from February 2022 to December 2022.
1. Preparation before the experiment
- To ensure the accuracy of study results, provide relevant training to rehabilitation therapists and assess their skills in advance to make sure that they can guide the children in the training.
NOTE: The rTMS technicians should be trained and qualified to ensure the safety of children. - Conduct rTMS safety screening with parents before the experiment, including questioning them about evidence of seizures and medications taken.
NOTE: Medications can lower the seizure threshold.
2. Recruitment
- Recruit children with SCP whose clinical diagnosis and classification meet the criteria of China Cerebral Palsy Rehabilitation Treatment Guidelines (2022)21.
- Ensure that the children are between 3 and 6 years old.
- Ensure that the children have Gesell Developmental Diagnostic Scale (GDDS) adaptive behavioral area development quotient (DQ) > 55 so that they can actively participate in training.
- Ensure that the children have Gross motor function classification (GMFCS) I-III.
- Ensure that the children can walk more than 10 m independently or with a walker.
- Exclude the following: children with other types of CP; children scheduled for medical rehabilitation or surgery during the study period; children with epilepsy, severe intellectual impairment, visual impairment, or attention deficit; children with cochlear implants or intracranial implants.
- Before the training, obtain informed consent forms from children's guardians for voluntary participation in this training program 1x a day, 5 days per week for 12 weeks.
3. Pretreatment assessment
- Analyze the baseline data collected from recruited children with SCP, including name, sex, age, cerebral palsy spasticity type, GMFCS, cognitive level, ankle foot orthosis wear, previous or current medical treatment, and surgical history.
- Rehabilitation assessment
NOTE: Studies have shown that the Comprehensive Spasticity Scale (CSS) used to assess the degree of lower limb spasm in children with SCP has good reliability and validity22.- Determine the degree of spasm by examining the lower limb Achilles tendon reflex, the muscle tension of the ankle plantar flexor group, and the ankle clonus. Use the following evaluation criteria: no spasm, <7; mild spasm, 7-9; moderate spasm, 10-12; and severe spasm, 13-16.
- Assess balance function according to the Pediatric Balance Scale (PBS)23, which includes 14 tested items. Each item is divided into five levels with 0-4 points for each item and 56 points in total. The higher the score, the better the balance function.
NOTE: PBS is based on the BBS Children's Revision, mainly adjusting the order of the tested items, shortening the time for maintaining posture, and clarifying test instructions. - Assess the children's walking ability based on the 10 m walking speed (10MWS)24.
- Ask children to walk as fast as possible on a runway with specifications of width x length =20 cm x 15 m, independently or wearing an ankle-foot orthotic or using a walking aid for children with GMFCS class III.
- Ask children to start walking at the 15 m marker; start timing at 12 m, and stop at 2 m to measure the time taken for the middle 10 m. Ask the children to perform three consecutive 10MWT tests and calculate the walking speed (m/s).
NOTE: The functional level of the children was graded I-III according to GMFCS, meaning they have certain standing and walking ability. - Evaluate the gross motor function level of the children by selecting a standing position in area D (13 items) and walking, running, and jumping in area E (24 items) in the Gross Motor Function Measure (GMFM). Calculate the score according to the completion degree of each item (0-3 points) and get the total score of Zones D and E. The higher the score, the better the gross motor function.
- Calculate the efficacy rate using equations (1) and (2) and assess the clinical effectiveness of gross motor function interventions by measuring the difference in the scores from the GMFM-88E section before and after treatment.
Efficacy rate (%) = (1)
(1)
Efficacy rate = significant effective rate + effective rate (2)- Consider the outcome to be significantly effective if the efficacy rate is >50%.
- Consider the outcome to be effective if the efficacy rate is between 20% and 50%.
- Consider the outcome to be ineffective if the efficacy rate is <20%.
4. Therapeutic method
NOTE: Explain the principles and objectives of the training program, as well as possible adverse effects and safety issues during the training process, to the guardians of the children.
- Randomly divide the children with SCP into four different groups: a conventional group, a rTMS group, an AOT group, and a combination intervention group according to the numerical table method (16 cases in each group in this study).
- Ensure that all the children receive conventional rehabilitation treatment, based on which they will be given different rehabilitation treatment measures. The conventional group receives no other rehabilitation treatment; the rTMS group receives rTMS; the AOT group receives AOT; and the study group receives rTMS combined with AOT.
- Explain in detail to the families of the subject children the possibilities of their participation in training programs of conventional rehabilitation, rTMS, AOT, and combined interventions. Ensure that the researchers are blinded to the allocation of the subjects and are not involved in the assessment.
- According to the admission order of these children, generate a numerical list as a spreadsheet. Randomize into groups as follows: numbers 1, 5, 9… for the regular group; numbers 2, 6, 10… for the rTMS group; numbers 3, 7, 11… for the AOT group; and numbers 4, 8, 12… for the combined intervention group. To ensure privacy, use a curtain to provide each child with a separate space during each treatment session.
- Conventional rehabilitation
- Exercise therapy
- Explain the principle and purpose of exercise therapy to the guardians of the children and notify them that the duration of treatment is 30 min.
- According to their muscle strength rating, instruct the children to perform muscle strength exercises for the training of hip abductor muscles, hip posterior extensor muscles, and ankle dorsal extensor muscles, 10x per set and three sets per day.
- According to their balance function level, instruct the children to conduct balance training such as standing without support, standing with feet together, and standing on one leg, with a duration of 10 min each time.
- According to their walking ability, instruct the children to carry out walking training such as handholding, independent walking, and crossing obstacles, with a duration of 10 min each time.
- Hydrotherapy
- Explain the principle, process, and purpose of hydrotherapy to guardians of the children and notify them that the duration of treatment is 20 min.
- When using the special hydrotherapy machine for children, adjust the water temperature to an appropriate temperature of 37-38 °C.
- Ask the parents to help their children take off their clothes, put on waterproof swimming trunks and hydrotherapy collars, and then get them into the hydrotherapy machine.
- Click on the bubble bath button to start treatment and instruct the children to stand, turn around, and take steps alternately with both feet in the water.
- Massage treatment
- Have the children diagnosed first.
- Explain the effects of massage treatment to the guardians of the children and notify them that the duration of treatment is 30 min.
- Place the children in the prone position and apply alternating pinching and pushing techniques 5-10x along both sides of the coronary artery and the bladder meridian.
- Place the children in the prone position and press, using the end of the thumb, the acupuncture points of Futu, Liangqiu, Zusanli, Jiexi, Huantiao, Chengfu, and Wuizhong from the top down.
- Place the children in the supine or prone position and apply rhythmic lifting and pinching 10-20x with the thumb and other four fingers alternately on the quadriceps, hamstrings, and calf triceps muscle at the same time.
- Exercise therapy
- rTMS
NOTE: The physical therapist engaged in performing rTMS first participated in the training arranged by the manufacturer. For the safety of the participants, the therapist or other trained medical professionals must supervise the entire treatment process and inform the guardians in advance that the pulse generated by rTMS may cause temporary and mild pain and slight twitching of the face and limbs when it hits the scalp.- rTMS patient preparation
- At the first visit, let the physical therapist know about the basic information and medical history of the subject children.
- Explain the process of rTMS treatment and possible responses to the guardians of the children and notify them that the duration of treatment is approximately 30 min.
- Place the children in the supine or seated position, degrease their hands with medical alcohol, and choose a suitable positioning cap for each of them according to their head circumference. Place the naso-occipital line on the positioning cap on the median line of the participating children, and the crossing point of the naso-occipital line and the temporal-parietal line at the midpoint of the line between the eyebrow and the occipital posterior carina.
NOTE: The appropriate size should be selected according to their head circumferences. - Affix the recording electrode to the abdominal muscle of the abductor pollicis brevis of the participating children, the reference electrode to the tendon of the abductor pollicis brevis, and the bottom electrode to the wrist.
- rTMS operation preparation
- Start the computer application on the rTMS instrument, input the basic information and diagnoses of the participating children, and determine the treatment plan.
- The stimulation coil is a circular air-cooled coil, the center of which coincides with the contralateral M1 area corresponding to the identified abductor pollicis brevis. Place the coil at 45° to the scalp.
NOTE: The positioning cap was designed according to the electroencephalography (EEG) 10-20 electrode arrangement system, which could quickly locate the M1 region. - Select a stimulation intensity of 30% and stimulate the M1 region corresponding to the contralateral abductor pollicis brevis muscle by manual monopulse.
NOTE: During the treatment, the participating children should hold their position to avoid deviation of the stimulation target. - Observe the motor evoked potentials interface graph and gradually reduce the stimulation intensity. Define the RMT as the minimum stimulus intensity that will elicit this response if at least 5 out of 10 consecutive stimulations of the child's primary motor cortex (M1) induce a motor potential strength of more than 50 mV in the contralateral abductor hallucis brevis muscle (Figure 1A).
- Click on the confirm button, save the RMT record, and then enter the treatment parameter setting page.
- rTMS treatment
- Use the following settings to perform low-frequency stimulation on the M1 region of the undamaged cerebral cortex: stimulation frequency 1 Hz, stimulation intensity 80% RMT, stimulation number 10, stimulation time 10 s, the number of repetitions 80, and the total number of pulses 80025,26 (see Figure 1B).
- Use the following settings to perform high-frequency stimulation of the M1 region of the damaged cerebral cortex: stimulation frequency 5 Hz, stimulation intensity 100% RMT, stimulation number 15, stimulation time 3 s, repetition times 80, and the total number of pulses 1,20010(see Figure 1C).
- Observe the responses of the participating children. For example, if the children start crying due to scalp beating, have excessive facial twitching, or show signs of a seizure and other adverse reactions, stop the treatment immediately.
NOTE: For children with spastic diplegia/quadriplegia, high-frequency stimulation of the M1 region of the damaged cerebral cortex was performed alternately on both sides of the damaged brain. For those with spastic hemiplegia, the M1 region of the undamaged cerebral cortex was stimulated at a low frequency, while the damaged cerebral cortex of M1 area was stimulated at a high frequency.
- rTMS patient preparation
- AOT
NOTE: AOT requires physical therapists to video subjects' body movements in advance and supervise the safety and training accuracy of the whole treatment process.- Explain the principle, process, and precautions of AOT to the guardians of the children, and notify them that the duration is 30 min.
- Have two professional physiotherapists shoot videos of body movements from three different angles: front, side, and back, and design six body movements for the purpose of improving lower limb balance and walking function.
- The first movement goes from sitting to standing: move the body forward from the upright sitting position by lifting the pelvis and extending the knee joint, gradually converting to the standing position, and then sit down. Perform this 3x consecutively (Figure 2A).
- The second movement is a standing exercise: move the body weight to the left or right as far as possible and then back to the neutral position. Perform it 3x in turn (Figure 2B).
- The third movement is also a standing exercise: move the body weight forward or backward as far as possible and then return to the neutral position. Perform it 3x in turn (Figure 2C).
- The fourth movement is also a standing exercise: rotate the body to the left or right as far as possible and then return to the neutral position. Perform it 3x in turn (Figure 2D).
- The fifth movement is a standing exercise: walk sideways to the left or right and then return to the neutral position. Perform it 3x in turn (Figure 2E).
- The sixth movement is a standing exercise: alternately step up or down a 10 cm high step with the left and right feet. Perform it 3x in turn (Figure 2F).
- Get the children gathered in a quiet room and sitting 5 m away from an 86 inch TV in comfortable positions.
- Have the physiotherapist explain the body movements first so that the children can then focus on watching the video.
- After watching the video, ask the children to imitate these movements.
5. Post treatment evaluation
NOTE: The pretreatment and 12 week post treatment evaluation for each patient would be completed by the same pediatric rehabilitation doctor.
- After 12 weeks of different rehabilitation measures for the four groups of children, have the same pediatric rehabilitation doctor re-evaluate the clinical efficacy of CSS, PBS, 10 MWS, GMFM, and gross motor function.
- Record the guardians' satisfaction and feedback on the treatment plan, including the degree of enjoyment of the treatment and improvement in self-awareness, as well as their wishes and suggestions for continuing the treatment.
6. Statistical analysis
- Enter the demographics, CSS, PBS, 10 m walking speed (10MWS), GMFM, and effective rate (%) assessment data into the software for statistical analysis.
- Analyze the counting data using the χ2 Test or Fisher Probabilistic Precision method.
- Determine whether the data conform to a normal distribution and express normally distributed data as mean ± SD.
- Use repetitive measurement deviation analysis for comparison among the four groups and perform repeated measures analysis of variance under the mixed model to verify whether the results and variation scores of each group are consistent with the approximately normal distribution.
- Consider time as an intra-group factor and intervention an inter-group factor. If there is any interaction between these two factors, test the inter-group difference at each time point at a= 0.05. If there is no interaction effect, test the main effect. Consider differences to be statistically significant at P < 0.05.
This paper presents the results of 64 children with SCP (Supplementary Table S1 and Supplementary File 1), who were randomly divided into four groups according to the numerical table method and given different rehabilitation measures for 12 weeks. During the entire process, the participating children had no adverse reactions such as headaches, dizziness, and seizures.
The demographic data of the four groups of children are shown in Table 1. Before treatment, there were no significant differences in the sex ratio, age, spastic category of cerebral palsy, GMFCS, GDDS developmental quotient (GDDS DQ), and usage of assistive devices (ankle foot orthosis or walker) (all P > 0.05).
The CSS scores of the four groups of children before and after the 12-week treatment have been compared in Table 2. After 12 weeks of training, the CCS scores of all four groups significantly decreased, with the combination intervention group showing significantly greater changes than the other three groups. The time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05).
The scores of PBS, 10MWS, and GMFM before and after the 12-week training of the four groups are shown in Table 3, Table 4, and Table 5. Compared to the pretraining scores, the scores of PBS, 10MWS, and GMFM of all four groups significantly increased after the treatment, with the scores of the combination intervention group improving the most. The time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05).
The clinical effects on gross motor function in all four groups of children are represented in Table 6. The total efficacy rate of gross motor function in the combination intervention group was 87.50%, which was significantly higher than those of the remaining three groups (rTMS group 62.50%, AOT group 68.75%, conventional group 25.00%) (χ2 = 13.850, P = 0.003).

Figure 1: Stimulation of the M1 area. (A) Threshold determination: The value of RMT was measured when the contralateral M1 region corresponding to the abductor pollicis breve muscle, which was stimulated with a single pulse to generate a motion-evoked potential. (B) Low-frequency stimulation on the M1 region of the undamaged cerebral cortex: stimulation frequency was 1Hz, stimulation intensity was 80% RMT, stimulation number was 10, stimulation time lasted for 10 s, the number of repetitions was 80 times, and the total number of pulses was 800. (C) High-frequency stimulation of the M1 region of the damaged cerebral cortex: stimulation frequency was 5 Hz, stimulation intensity was 100% RMT, stimulation number was 15, stimulation time lasted for 3 s, repetition times was 80 times, and the total number of pulses was 1,200. Please click here to view a larger version of this figure.
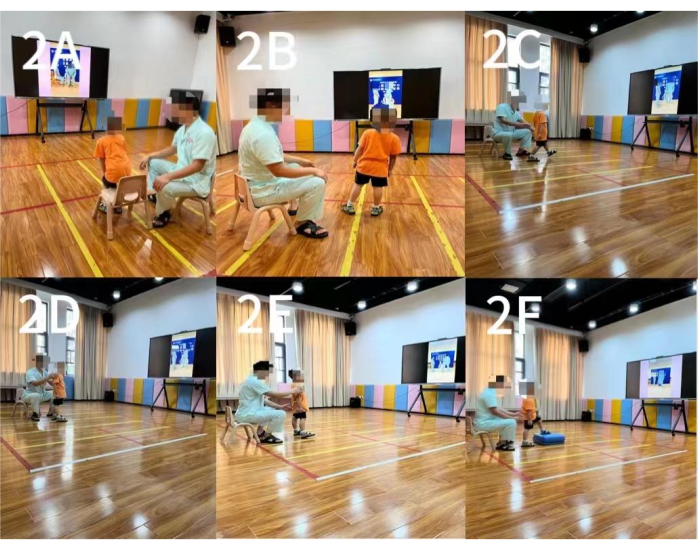
Figure 2: Action observation training. (A) The first movement: Sit-to-Stop Conversion. (B) The second movement: left/right bodyweight shifting. (C) The third movement: back/forth bodyweight shifting. (D) The fourth movement: left/right body rotation. (E) The fifth movement: left/right walking. (F) The sixth movement: stepping up/down alternatively. Please click here to view a larger version of this figure.
| (n=64, x±s) | |||||||||
| Item | Conventional Group | rTMS Group | AOT Group | combination intervention group | χ2 /F | P | |||
| Number (n) | 16 | 16 | 16 | 16 | |||||
| Sex Ratio (Male/Female) | 10/6 | 10/6 | 13/3 | 9/7 | 2.494 | 0.476 | |||
| Age (Year) | 4.44±0.80 | 4.74±0.68 | 4.71±0.54 | 4.63±0.68 | 0.654 | 0.683 | |||
| Classification of spastic cerebral palsy (spastic hemip legia/spastic dip legia/spastic quadriplegia) | 02-07-2007 | 5/10/1 | 6/9/1 | 5/10/1 | 2.105 | 0.945 | |||
| GMFCS (n) (Level I/II/III) | 7/3/6 | 6/5/5 | 8/5/3 | 8/5/3 | 2.750 | 0.868 | |||
| GDDS DQ | 70.06±10.25 | 70.13±9.44 | 71.56±12.58 | 69.25±6.89 | 0.148 | 0.931 | |||
| Usage of assistive devices (n) Yes/No |
5/11 |
3/13 | 3/13 | 4/12 | 1.780 | 0.699 | |||
Table 1: Comparison of the basic information of the four groups of children (n = 64, x ± s). *One-way analysis of variance. Before the training, there were no significant differences in sex ratio, age, spastic category of cerebral palsy, GMFCS, GDDS developmental quotient (GDDS DQ), and usage of assistive devices (ankle foot orthosis or walker), indicating comparability. Abbreviations: GMFCS = Gross motor function classification; GDDS DQ = Gesell developmental diagnosis schedule developmental quotient.
| Group | Number (n) | BEFORE | AFTER | F | P | ||
| Conventional Group | 16 | 10.63±1.67 | 10.19±1.76 | ||||
| rTMS Group | 16 | 10.88±1.41 | 9.75±1.13 | ||||
| AOT Group | 16 | 10.75±1.13 | 9.75±1.00 | ||||
| combination intervention group | 16 | 10.69±1.01 | 8.88±1.02 | ||||
| Group Factor | 0.774 | 0.513 | |||||
| Time Factor | 228.261 | <0.001 | |||||
| Group Factor * Time Factor | 15.217 | <0.001 | |||||
Table 2: Comparison of CSS scores in the four groups of children (n = 64, x ± s). After treatment, repeated-measures ANOVA results showed that the time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05). Abbreviations: CSS = Comprehensive Spasticity Scale; rTMS = repeated transcranial magnetic stimulation; AOT = action observation training.
| Group | Number (n) | BEFORE | AFTER | F | P | ||
| Conventional Group | 16 | 28.25±9.38 | 31.13±9.22 | ||||
| rTMS Group | 16 | 29.44±10.05 | 35.56±9.82 | ||||
| AOT Group | 16 | 29.25±9.84 | 35.94±8.62 | ||||
| combination intervention group | 16 | 29.81±11.59 | 41.88±8.03 | ||||
| Group Factor | 1.12 | 0.348 | |||||
| Time Factor | 371.208 | <0.001 | |||||
| Group Factor * Time Factor | 27.954 | <0.001 | |||||
Table 3: Comparison of PBS scores in the four groups of children (n = 64, x ± s). After treatment, repeated-measures ANOVA results showed that the time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05). Abbreviations: PBS = Pediatric Balance Scale; rTMS = repeated transcranial magnetic stimulation; AOT = action observation training.
| Group | Number (n) | BEFORE | AFTER | F | P | ||
| Conventiona Group | 16 | 1.02±0.14 | 1.10±0.16 | ||||
| rTMS Group | 16 | 0.98±0.18 | 1.15±0.16 | ||||
| AOT Group | 16 | 0.99±0.12 | 1.15±0.09 | ||||
| combination intervention group | 16 | 1.02±0.15 | 1.24±0.11 | ||||
| Group Factor | 0.946 | 0.424 | |||||
| Time Factor | 501.551 | <0.001 | |||||
| Group Factor * Time Factor | 19.275 | <0.001 | |||||
Table 4: Comparison of 10MWS scores in the four groups of children (n = 64, x ± s). After treatment, repeated-measures ANOVA results showed that the time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05). Abbreviations: 10MWS = 10 m walking speed; rTMS = repeated transcranial magnetic stimulation; AOT = action observation training.
| Group | Number (n) | BEFORE | AFTER | F | P | ||
| Conventiona Group | 16 | 46.63±20.05 | 54.00±22.19 | ||||
| rTMS Group | 16 | 48.94±19.96 | 61.94±20.61 | ||||
| AOT Group | 16 | 50.25±15.25 | 63.63±16.40 | ||||
| combination intervention group | 16 | 50.94±18.43 | 75.69±17.86 | ||||
| Group Factor | 1.300 | 0.283 | |||||
| Time Factor | 502.502 | <0.001 | |||||
| Group Factor * Time Factor | 31.184 | <0.001 | |||||
Table 5: Comparison of GMFM scores in the four groups of children (n = 64, x ± s). After treatment, repeated-measures ANOVA results showed that the repeated-measures ANOVA results showed that the time effect and the interaction effect between groups and time were significant (P < 0.05), while the effect between groups was not significant (P > 0.05). Abbreviations: GMFM = gross motor function measure; rTMS = repeated transcranial magnetic stimulation; AOT = action observation training.
| Group | Number | obvious effective | Effective | Ineffective | Effective rate | ||
| Conventional Group | 16 | 1 | 3 | 12 | 25.00% | ||
| rTMS Group | 16 | 3 | 7 | 6 | 62.50% | ||
| AOT Group | 16 | 2 | 9 | 5 | 68.75% | ||
| combination intervention group | 16 | 7 | 7 | 2 | 87.50% | ||
| χ2 | 13.850 | ||||||
| P | 0.003 | ||||||
| Abbreviations: rTMS = repeated transcranial magnetic stimulation; AOT = action observation training. | |||||||
Table 6: Comparison of gross motor function of all four groups of children (n [%]). Abbreviations: rTMS = repeated transcranial magnetic stimulation; AOT = action observation training.
Supplementary File 1: Case information of a patient. The patient was treated with rTMS combined with AOT. After 12 weeks of treatment, the data of various evaluation indicators before and after treatment were compared to determine the clinical effect of the combined intervention on the patient's gross motor function. Please click here to download this File.
Supplementary Table S1: Patient data. Please click here to download this File.
