In this protocol, we successfully establish a rat femoral box-cavity defect model with dimensions of 4.5 mm x 1.5 mm by drilling. In order to analyze the healing process, we collected the femoral tissue on the operated side at 0 days, 2 weeks, 4 weeks, and 6 weeks after surgery, which are the key time points of endochondral ossification, intramembranous ossification, and bone remodeling during the healing process of femoral trauma in rats2. On post-operative day 0, reconstruction of the 3D model from micro-CT bitmap data showed that we successfully modeled a box-cavity defect in the femur with a size of 4.5 mm x 1.5 mm deep to the marrow cavity (Figure 3A). Results of micro-CT showed mineralized trabecular bone formation in the interstitial space of the cortical bone defect 2 weeks after model creation (Figure 3B). The surface of the new bone tissue in the defect area showed mature, dense cortical bone, and trabecular bone tissue was still visible on the medullary side 4 weeks postoperatively (Figure 3C). After 6 weeks, the defect area was almost composed of mature, dense cortical bone, with only a small amount of trabecular bone tissue remaining near the medullary side, indicating that the defect area had basically healed (Figure 3D).
We also analyze the collected specimens by H&E staining and Masson trichrome staining (Figure 4). The results showed that naïve trabecular-like bone tissue was formed in the defect area 2 weeks postoperatively, and the periosteum around the defect area thickened and connected with the newborn trabecular bone tissue in the defect area (Figure 4A,A',B,B'). At 4 weeks after creating the defect, dense cortical bone tissue was formed on the surface of the defect area and connected with the cortical bone on both sides of the defect; trabecular-like bone tissue was resorbed heavily on the medullary side (Figure 4C,C',D,D'). Mature cortical bone tissue was formed in the defect area, and the trabecular bone tissue on the medullary side was almost completely resorbed 6 weeks postoperatively (Figure 4E,E',F,F'), indicating that the defect's healing process was almost complete.
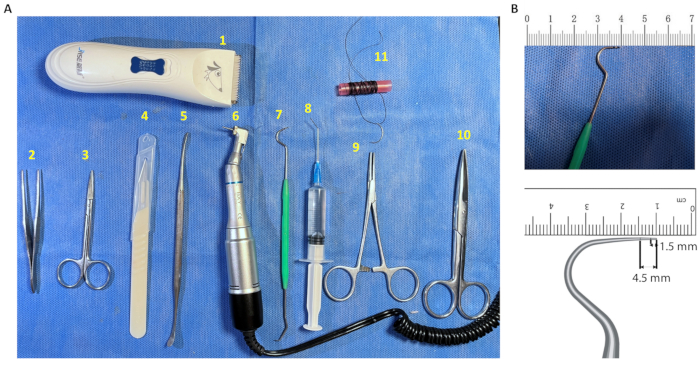
Figure 1: Instruments required for defect creation. (A) Surgical instruments. (1) Electric shaver; (2) Ophthalmic forceps; (3) Ophthalmic scissors; (4) Disposable scalpel; (5) Periosteal separator; (6) Oral low-speed handpiece; (7) Modified oral probe; (8) Disposable irrigation vac; (9) Needle holder; (10) Tissue scissors; (11) 3.0 suture. (B) Oral probes labeled with the dimensions of the defect diameter. The large curved end of the sterile disposable oral probe was marked with a 1.5 mm and 4.5 mm scale for intraoperative measurement of the diameter of the defect area. Please click here to view a larger version of this figure.
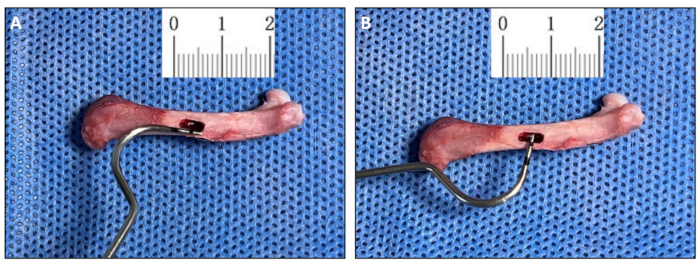
Figure 2: Morphology of the box cavity defect (Day 0). (A,B) Measurement of Day 0 post-surgery samples using a modified oral probe that was used to create the box cavity defect (4.5 mm x 1.2 mm). Please click here to view a larger version of this figure.

Figure 3: Micro-CT analysis of the healing process of the defect area. 3D reconstructed images of the defect area at 0 days, 14 days, 28 days, and 42 days after surgery. (A) Longitudinal plane . (B–D) Longitudinal (left panel), sagittal (middle) and cross-sectional (right panel) micro-CT images of healing of the defect area at 14 days, 28 days, and 42 days. The yellow dashed box in A, B, C, and D represents the defect area. The yellow dashed line represents the edges of the defect, and the yellow arrow represents the new bone tissue in the defect area. Please click here to view a larger version of this figure.
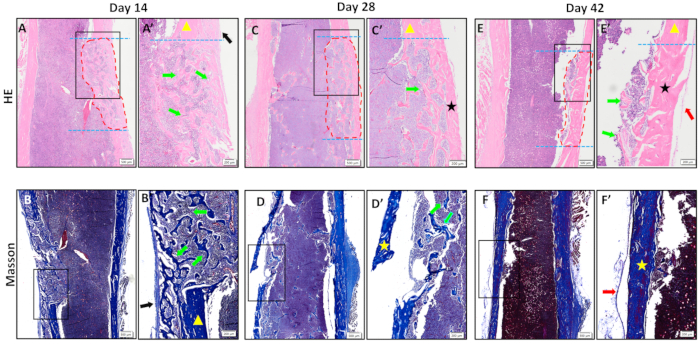
Figure 4. Histopathological results. (A-F) H&E and Masson staining of the defect area at 14 days, 28 days, and 42 days.(A'-F') The zoomed-in images of the black rectangular boxes shown in A-F.Trabecular-like mineralized bone tissue was formed in the defect area at 14 days after surgery; cortical bone tissue was formed on the surface of the defect area and connected to both ends of the defect area at 28 days after surgery; mature cortical bone tissue was formed in the defect area at 42 days after surgery, and healing was basically completed. The blue dotted line indicates the edge of the defect; the area circled by the red dotted line is the new bone tissue in the defect area; the black arrow is the thickened periosteum; the yellow triangle is the old cortical bone; the green arrow is the new trabecular-like bone tissue; the black and the yellow stars are the new cortical bone tissue; and the red arrow is the new periosteum. Scale bars: 500 µm (A-F), 200 µm (A'-F'). Please click here to view a larger version of this figure.
