Procedures involving animal subjects have been approved by the Chancellor's Animal Research Committee of the University of California, Los Angeles (ARC protocol number 2002-125), and the Animal Research: Reporting In Vivo Experiments (ARRIVE)22. For this method, eighteen 3-week-old C57BL/6J male mice were used and underwent dental extractions, implant placement and peri-implantitis induction. All dental procedures were performed under 10× microscopic magnification and carried out by trained and calibrated operators (Figure 1A).
1. Pre-extraction steps
- Perform the procedure in a surgical room complying with all biosafety and protection standards.
- Perform asepsis of all surfaces with triple friction using a 70% isopropyl alcohol solution.
- Anesthetize 3-week-old C57BL/6J male mice with 3% isoflurane. Check for the lack of response to paw withdrawing upon touch to ensure sufficient anesthetic depth is obtained.
- To avoid interfering with procedures in the mouth, use a nosecone to maintain isoflurane anesthesia.
- Have an auxiliary operator to stabilize the animal and maintain the mouth opening (Figure 1B).
- Apply ophthalmic lubricant, to prevent irritation in the eyes before starting the extraction.
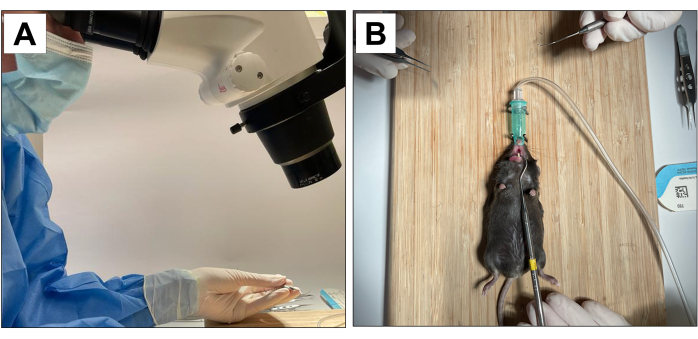
Figure 1: Operative adaptations: (A) Microscopic magnification. (B) Adapted inhalation anesthesia system and stabilization for mouth opening. Please click here to view a larger version of this figure.
2. Dental extraction
- For dental extractions, introduce a #5 dental explorer between the first and the second molar to start the elevation and luxation procedures by moving the instrument in the mesio-distal direction until the tooth moves in the socket (Figures 2A).
- Next, introduce the #5 dental explorer in the mesial site of the first molar. Do this by moving the instrument in the mesio-distal direction until the tooth moves in the socket.
- Following elevation, use the tip forceps and the suture tying forceps to remove the 1st molar.
- Next, introduce the dental explorer between the 2nd and 3rd molar to elevate and luxate the 2nd molar (Figure 2B).
- Then, use the tip forceps and/or the suture tying forceps to remove the tooth using the instruments to hold it and take out of the mouth. (Figure 2C).
- After dental extractions, ensure complete hemostasis achievement by using a sterile cotton tipped (Figure 2D) for 1 min (Figure 2E,F).
- Immediately after extraction, provide all animals with pain medication (Carprofen/Rimadyl 5 mg/kg) every 24 h. Administer the medication through subcutaneous injection.
- In addition, replace regular food with a soft diet. Administer the antibiotic (Amoxil 0.25 mg/mL) orally by incorporating the medication into the drinking water. Do this for four weeks after extractions.
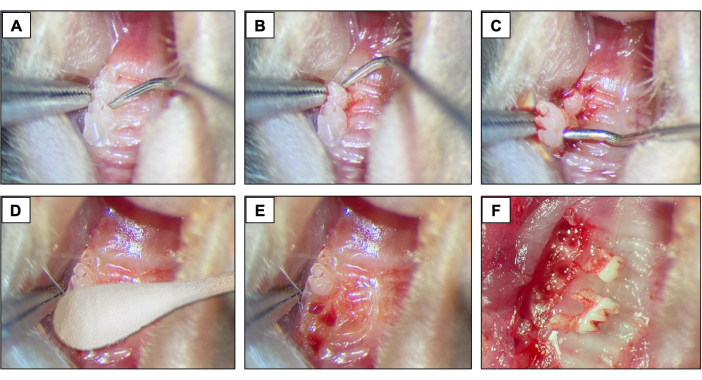
Figure 2: Initial extraction sequence: (A, B) Maxillary region with 1st and 2nd molar teeth and use of dental explorer for elevation and luxation. (C) Use of the tip forceps and explorer for luxation and tooth removal. (D) Hemostasis. (E, F) Alveolar appearance after extractions. Please click here to view a larger version of this figure.
3. Implant placement
- Using a 15c blade, create a mesio-distal incision through the keratinized tissue in the area corresponding to the previously present teeth. Use the right maxillary molars as a spatial reference (Figure 3A).
- Raise the buccal and palatal full-thickness flaps by using a #5 dental explorer, ensuring complete flap elevation (Figure 3B).
- Perform the osteotomy using a 0.3 mm diameter carbide micro hand drill attached to a Pin Vise (hand drill) and activate it in a clockwise rotation. Create osteotomy sites with approximately 1 mm deep into the healed extraction sockets (Figure 3C).
- Place the custom-designed screw-shaped implants with a smooth machined surface (1.0 mm long and 0.5 mm in diameter) fabricated from 6AL4V titanium rods (Figure 3D), one per animal, by self-tapping in the region of the first and second maxillary left molars using a clockwise screwing motion (Figure 3E-I).
- Immediately after implant placement, administer pain medication (Carprofen/Rimadyl 5mg/kg every 24 h) through subcutaneous injection.
- Allow the implants to heal for four weeks, during which time administer antibiotics and feed as previously described.
- At the end of the healing period, ensure that the mucosal wound is completely closed and has a light pink appearance.
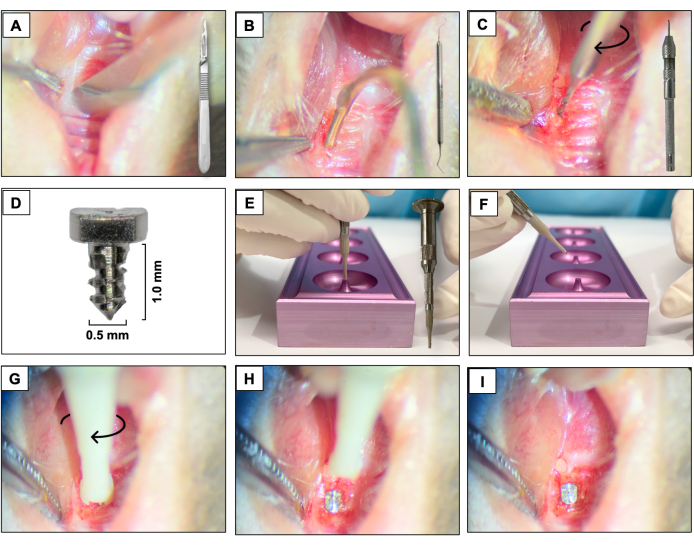
Figure 3: Implant placement sequence: (A) Incision using a 15c blade attached to the handle. (B) Full-thickness flaps using #5 dental explorer. (C) Osteotomy using a 0.3 mm carbide micro hand drill attached to a Pin Vise. (D) Titanium dental implant. (E, F) Implant support and implant holder. (G- I) Implant placement using a clockwise screwing motion. Please click here to view a larger version of this figure.
4. Peri-implantitis induction
- Place a silk ligature (6-0) around each fixture immediately apical to the implant head by contouring the surface of the implant and fixing it with a double knot. Keep the ligature for two weeks allowing the peri-implantitis development.
- Check the ligatures every two days to make sure they are still present. If missing, place a new ligature.
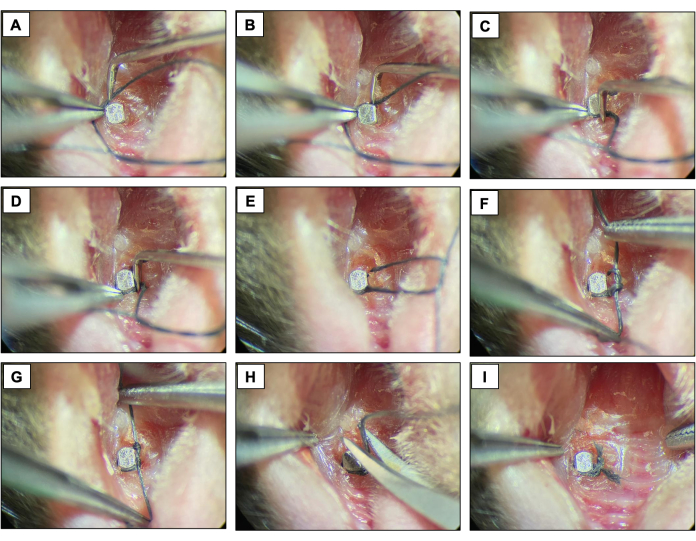
Figure 4: Ligature-induced peri-implantitis sequence. (A-D) Silk ligature (6.0) placed around the implant head. (E-G) Knot closure. (H) Ligature cut. (I) Final appearance. Clinical images obtained from live animals under sedation. Please click here to view a larger version of this figure.
5. Sacrifice
- After the peri-implantitis induction period (two weeks), sacrifice all animals with a high concentration of inhaled isoflurane, followed by a secondary method of cervical dislocation with a rod pressed into the base of the skull and quickly pulling the hind limbs, causing the separation of the cervical vertebrae from the skull.
- Separate the maxillae using sharp instruments, such as surgical scissors, that will separate the animal's entire jaw from the rest of the body.
- Photograph the maxillae using an optical microscope, fix it in 10% formalin for 24 h, then store in 70% ethanol.
6. Micro-computed tomography (µCT )
- Scan the maxillae as previously described18,19 using micro-computed tomography (micro-CT) scanning.
- Turn on the scanner and the computer, then open the scan software, click on the radiation sign, and wait 15 minutes to preheat it.
- Open the equipment door by clicking on the door icon.
- Use a quarter-size rotary table. Place the maxilla on a 15ml conical tube. Fix the tube in the rotary table base. Place the rotary table in the equipment screw.
- Close the equipment door by clicking on the door icon.
- Turn on the X-Ray source.
- Click on the grab image icon and make sure the bone is on the field.
- Adjust a resolution of 10 µm pixel size, X-ray energy of 55 KVp and 181 µA, filter of AI 0.5 mm, rotation step 0.4, average frame 10. These settings will generate an estimated scanning time of 24 minutes.
- Start the acquisition.
- For reconstruction open the reconstruction software. Use beam hardening of 20%. Use ring artifact of 5%. Use a dynamic range of 0-0.13. Deselect label ON. Click on Preview. Choose the adequate view that is seen for the region of interest, and save it as TIFF.
- Orient the images obtained using software for viewing and analyzing data. Make the long axis of the implant head parallel to the sagittal and coronal axes and perpendicular to the axial axis.
- Save the sagittal image as a single image for linear bone analysis.
- Save transaxial image as a dataset for volumetric bone analysis.
- Perform linear bone analysis using the analyzing data software. Measure the distances in millimeters between the implant head and the alveolar bone in the sagittal and coronal planes, including mesial, distal, buccal, and palatal sites.
- Perform volumetric bone analysis using analyzing data software. Track bone loss around implants by drawing the region of interest in all slides corresponding to the bone loss.
7. Statistical analysis
- Measure linear and volumetric microtomographic bone loss and normalize these values by dividing each value by the average of the control group. Present an average for all groups, as mean ± standard error of the mean (SEM).
- Compare significance using a two-way analysis of variance (ANOVA) followed by a Tukey's test with a 95% confidence interval. (Prism 5). Apply significance levels as follows: p≤0.01**, p≤0.001****.
For this method, eighteen 3-week-old C57BL/6J male mice were used and underwent dental extractions, implant placement and peri-implantitis induction. There were nine animals per group which was statistically significant, considering linear bone loss achieving 80% power, 15% standard deviation (σ) and 95% confidence interval (α =0.05). Mice were fed a soft diet ad libitum during the experiment. Nine mice received a ligature (ligature-induced periimplantitis-experimental group), and nine mice did not receive ligature (control group).
The success rate of implant osseointegration
Respecting the four-week healing period and observing the clinical stability, implants in our study had high survival and 100% success rates as none of the placed implants was lost. No other adverse events were observed.
Clinical evaluation
Using optical microscopy, clinical evaluation was performed through visual inspection and clinical photos immediately after sacrificing the mice (Figure 5). When compared to the control group, inflammation, pocket formation and increased soft tissue edema was observed around the implant in the peri-implantitis group. No evidence of severe clinical phenotype complications was observed.
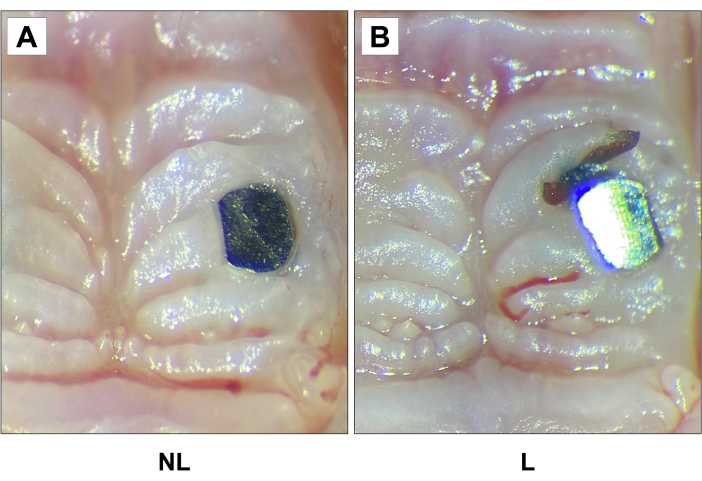
Figure 5: Representative clinical images of (A) non-ligature (NL) and (B) ligature (L) groups 2 weeks after ligature. Increased soft tissue edema was observed around the implant in the peri-implantitis group compared to the other group. 20X magnification. Please click here to view a larger version of this figure.
Microcomputed tomography analysis (µCT)
Two weeks after ligature placement, when comparing non-ligature and ligature groups, there were significant differences in bone height observed via by linear analysis (Figure 6A, B and C), and bone loss volume observed via volumetric analysis (Figure 6D). Linear bone loss in the ligature-induced PI group was significantly increased compared to the control group. Likewise, when comparing the volumetric bone loss, the PI group showed more significant circumferential bone loss compared to the control group.
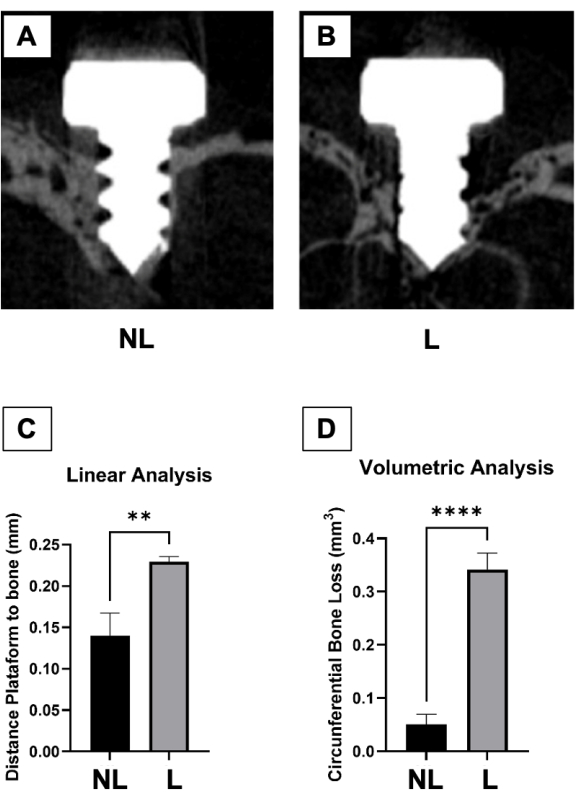
Figure 6: Micro-computed tomography analysis. (A) Representative microtomographic sections of control (non-ligature – NL) and (B) peri-implantitis (ligature – L) groups. (C) Graph represents the averaged distance from the implant head to the alveolar bone 2 weeks after ligature. (D) The graph represents the average circumferential volumetric bone loss 2 weeks after ligature. Data represented as average SEM. *p<0.05 (n≥5 for all groups/time points). Please click here to view a larger version of this figure.
Histological evaluation
To determine cellular changes, including bone loss around the implant, decalcified samples were sectioned and stained with hematoxylin & eosin (HE) (Figure 7). The decalcification process was carried out by immersing the samples in 15% ethylenediaminetetraacetic acid (EDTA), pH 7.4, for four weeks, changing the solution every three days. With the implants removed, the specimens were embedded in paraffin. So, 5 µm-thick sagittal dimensioned paraffin sections were stained with HE, following standard protocols. As a result, more apical epithelial migration, moderate cellular infiltration, and bone loss in peri-implantitis samples were observed when compared to the control group.
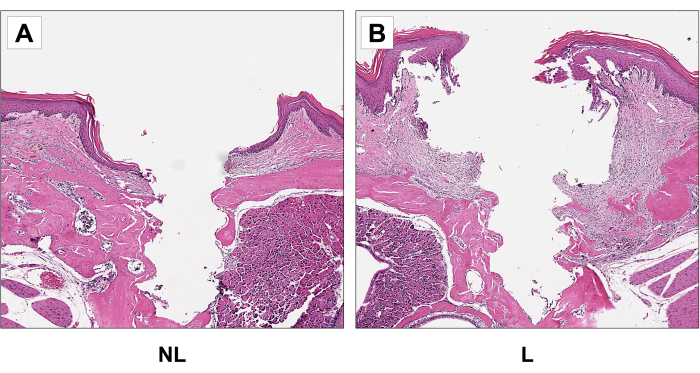
Figure 7: Representative sagittal H&E images of non-ligature (NL) (A) and (B) ligature (L) groups. Increased apical epithelial migration and bone loss in the ligature group compared to the control group. 20x magnification. Please click here to view a larger version of this figure.
According to the most recent consensus on the classification of peri-implant diseases and conditions, the peri-implantitis diagnosis requires bone loss beyond crestal bone level changes resulting from initial bone remodeling22. Therefore, our study presents well-established and validated peri-implantitis diagnosis parameters. And offer a comprehensive evaluation of the condition under investigation.
