Decision-making is an important component of human executive function, one in which a choice about a course of action is made from many possibilities.
For instance, a person’s ability to obtain a beverage could result from making good decisions, like choosing to go to the cash register and pay for it, or poor ones, such as running out the door without paying.
This latter example—the risky act of stealing—is considered an undesirable decision, one that occurs as a result of damage to the frontal lobes—and in particular, the ventromedial prefrontal cortex, VMPFC for short.
This video demonstrates how to design and execute the Iowa Gambling Task—a highly sensitive measure of complex decision-making ability—where individuals must integrate information about losses and gains over the course of a high-risk card game.
In this experiment, two groups of participants—patients with known damage to the VMPFC and controls, individuals without such damage—perform the Iowa Gambling Task, which examines decision-making ability dealing with reward and punishment.
All are shown four decks—labeled A through D—that contain identical-looking cards and given play money to use, as the overall goal is to maximize profit.
During each turn, participants choose one card from any of the four piles and subsequently receive a certain amount of predetermined money that only the researcher knows.
For instance, they might pick a card that results in not only winning money but also losing some. Or, they may even lose more than they win. The trick then is to understand the risk associated with every deck.
Although A and B yield greater rewards than C and D, they also result in higher penalties and thus, lead to losses in the long term. Decks A and B result in the same long term losses, but the punishment in A is more frequent and of lower magnitude than in B.
Overall, choosing from A and B will result in net losses, while choosing from C and D will result in net gains, which is why sets A and B are referred to as bad, and C and D as good.
Thus, to make advantageous choices, participants must integrate information about losses and gains over time and avoid the bad sets.
The dependent variable here is the number of card turns the participant makes from each of the four decks.
Based on previous work by Bechara, Damasio, and colleagues, patients with VMPFC damage are expected to make more selections from the bad ones—A and B—and avoid choosing from the good—C and D—mimicking their real-life inability to make valuable decisions.
For the purpose of this demonstration, test a patient with known cortical damage. Note that their data will be compared to those collected from controls without brain damage, who are also matched in age and intellect.
In preparation for the task, seat the patient at a table in front of four decks of identical-looking cards, and hand them $2000 in play money.
Instruct them that they must choose one card at a time from any of the four piles, and after flipping each card, they will receive a certain amount of money.
Further inform them that they are free to switch between decks at any time, as often as they want, and to take their time, in order to maximize their profit on the loan money.
Begin by having the patient make their first selection, and announce the amount of the reward or penalty according to the scorecard. Give them the amount of play money that they earn, and tell them to hand back any money they have lost before proceeding to the next turn.
Keep track of every card turn by marking the appropriate cell of the scorecard. In the event that a deck is completed before the experiment is over, notify the patient that they can now only choose from the three remaining decks. End the task when 100 cards have been turned.
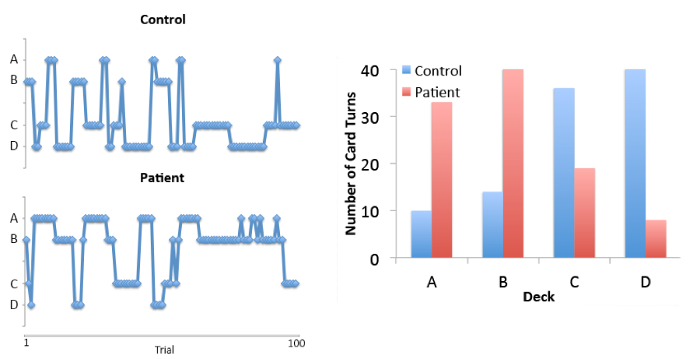
To examine participants’ decisions over time, plot the deck selections across the course of the 100 trials—separately for controls versus patients with VMPFC damage.
While controls initially sampled from the bad decks, they eventually learned to avoid them. Patients, on the other hand, continued to sample from the bad ones throughout the experiment.
To make group comparisons, summarize these data into a bar graph, where the total number of card turns is plotted across decks.
Notice how normal controls made more selections from the good decks—C and D—and avoided the bad—A and B. On the other hand, patients with VMPFC damage made more selections from the bad sets, and largely avoided the good ones.
These results indicate that patients with frontal brain damage perform differently in this task compared to healthy controls, such that they more frequently draw from the high reward/high punishment decks, even though those decisions result in long-term losses.
Now that you are familiar with using the Iowa Gambling Task to quantify risky outcomes in patients with frontal lobe damage, let’s look at how the paradigm can be used to assess decision-making in a variety of populations, including individuals with amygdala damage and those diagnosed with schizophrenia.
While the role of the PFC in decision-making is well studied, other brain regions contribute to implementing advantageous versus disadvantageous choices.
Given the amygdala’s role in processing incentive stimuli, damage to this region would likely disrupt the integration of reward and punishment states vital to the gambling task.
Using a similar paradigm, researchers have shown that patients with bilateral amygdala damage also show severe decision-making impairments.
Just like patients with VMPFC damage, individuals with schizophrenia also choose from bad decks; however, they show a distinctive pattern of choices, making more selections from the low frequency but high magnitude losses—decks B and D.
These results indicate that schizophrenic patients are sensitive to reward versus punishment, but fail to advantageously take into account the magnitude of the punishment.
Thus, the Iowa Gambling task can be used to reveal a range of cognitive contributions to decision-making that may be associated with different underlying deficits.
You’ve just watched JoVE’s introduction to quantifying decision-making in the laboratory using the Iowa Gambling Task. Now you should have a good understanding of how to administer this paradigm by observing and responding to different card choices, as well as how to analyze and interpret the results.
Thanks for watching!