Outcomes for the evaluation of craniofacial VML and tissue regeneration using biomaterials include both quantitative and qualitative outcomes.
Figure 2 depicts an example of qualitative evaluation using the previously described model. The observation of de novo muscle fiber growth within our hydrogel is a qualitative positive outcome (Figure 2A) and suggests a biomaterial can provide sufficient architectural support and growth factor or nutrient delivery. Retention of hydrogel within the wound bed (Figure 2B) is visible on HE stain. Qualitative assessment of other tissues within a biomaterial may be done, such as the identification of blood vessels using HE (Figure 2C) and Masson's trichrome (Figure 2D). The mandibular and buccal branches of the facial nerve are visible on the upper left and upper right corners of the image in Figure 2B, confirming the correct placement of hydrogel in the VML injury bed and providing orientation. A layer of fascia is seen above the hydrogel, confirming the fascial closure was successful and remained intact during the postoperative period. A negative result seen in this stage would include full loss of hydrogel (Figure 2E) or loss of fascial closure and extrusion from the wound bed (Figure 2F), with HE showing evidence of a wound bed or fibrotic scar depending on the elapsed time postoperatively.
Immunohistochemical analysis is critical in the evaluation of biomaterials for the treatment of craniofacial VML in order to identify cell types and molecular interactions at the cellular level. Because VML results in the loss of resident cells and architecture capable of regenerating the skeletal muscle, de novo muscle regeneration at the injured site is an important outcome in treatment4 and the evaluation of efficacy in biomaterials-based therapies for VML. Developmental isoforms of myosin, including embryonic (MYH3) and neonatal myosin (MYH8), are re-expressed in regenerating skeletal muscle fibers and provide a specific marker for regenerating fibers18,19. Figure 3 shows an example of how immunohistochemistry can be used to identify cellular types of interest, in this case, the embryonic myosin heavy chain.
Finally, ImageJ can be utilized to quantify features of histology slides, including immunohistochemistry and specialized stains such as Masson's trichrome, to measure the fibrotic response (Figure 4). Removal of a portion of muscle in VML injuries changes the muscle architecture and composition, leading to increased collagen I deposition and gross compartmental tissue fibrosis2,3. Many studies evaluating biomaterials-based treatments for VML compare fibrosis between their intervention group and control groups4. Using the method described here, the wound beds in animals that underwent VML injury can be identified on Masson's trichrome as fibrotic scars (Figure 4A). Color deconvolution through ImageJ can isolate and quantify the blue channel corresponding to connective tissue (Figure 4B), then set to grayscale for measurement (Figure 4C). The area of the scar can be isolated and measured using Image J (Figure 4D) and calibrated to a scale bar on the image for accurate size and reproducible area. Using this approach, the connective tissue deposition can be measured (Figure 4E).
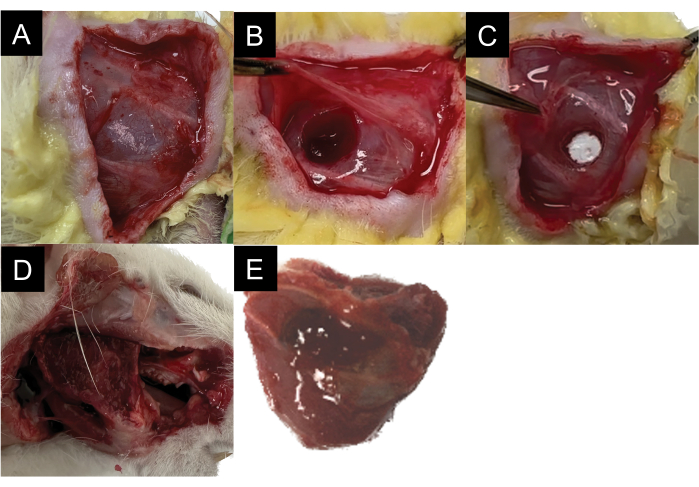
Figure 1: Surgical schematic demonstrating the steps. (A,B) Surgical masseter VML injury. (C) Biomaterial application. (D) Masseter harvesting. (E) Muscle morphology following harvesting. Please click here to view a larger version of this figure.
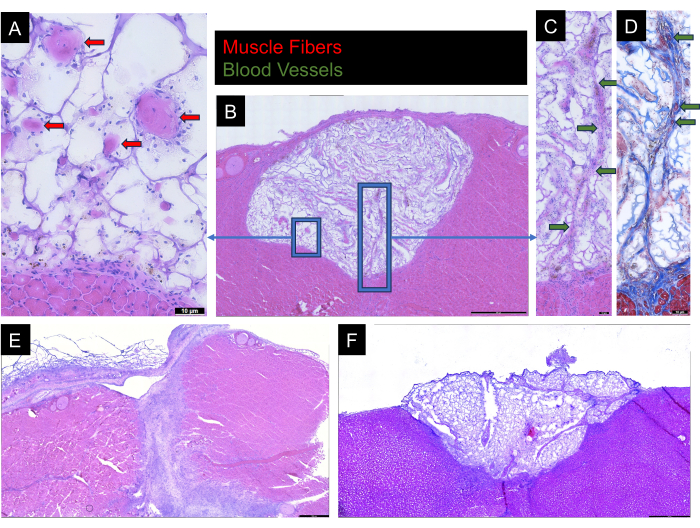
Figure 2: HE and Masson's trichrome staining. (A) HE-stained rat masseter sections from hydrogel-muscle interface with arrows indicating structures morphologically identified as skeletal muscle fibers. (B) HE-stained rat masseter section demonstrating the abundance of skeletal muscle fibers throughout hydrogel. (C) HE-stained and (D) Masson's trichrome-stained tissue with arrows indicating structures morphologically identified as blood vessels. (E,F) Negative results showing full loss of hydrogel with gel adhered to the superficial aspect of the masseter rather than the wound bed and incomplete loss of hydrogel with loss of fascial closure, respectively. Please click here to view a larger version of this figure.
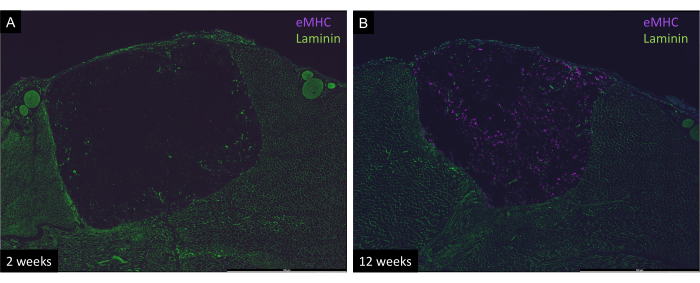
Figure 3: Immunohistologic staining for embryonic myosin heavy chain (eMHC) and laminin on rat masseter cross sections. (A) 2 weeks post-surgery. (B) 12 weeks post-surgery. An increased concentration of eMHC is seen in the 12-week sample relative to the 2-week sample. Images captured at 20x magnification. Please click here to view a larger version of this figure.
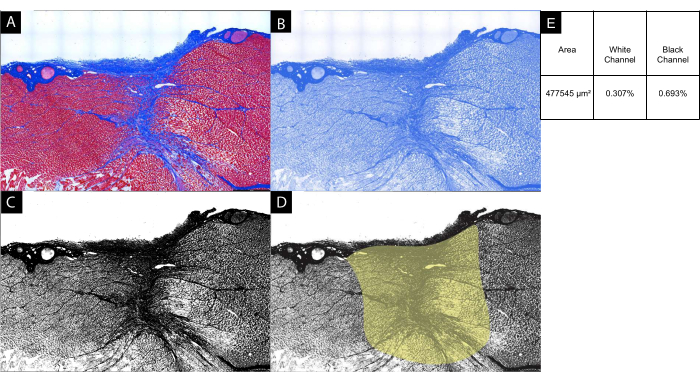
Figure 4: Quantitative fibrosis analysis. (A) Masson's trichrome-stained rat masseter section for quantification of connective tissue deposition as a proxy for wound fibrosis after VML injury at 12 weeks. (B) Image J was used to deconvolute the blue channel corresponding to connective tissue. (C) The image was converted to grayscale for analysis. (D) The area corresponding to the fibrotic scar was isolated, and (E) the cross-sectional area and percentages of the field corresponding to white (background) and black (connective tissue) were calculated. Images captured using light microscopy at 10x magnification. Please click here to view a larger version of this figure.
